
{kind=link}
{kind=link}
{kind=link}
Varian promotes the Eclipse dose calculation algorithm AcurosXB as being ultrafast, which is certainly a strong claim. We tested the validity of this allegation by measuring the overall AXB calculation time (in plan dose and field dose mode, see sidebar) and comparing it to the time it takes AAA to calculate the same plan with the same spatial resolution.
Our current DCF
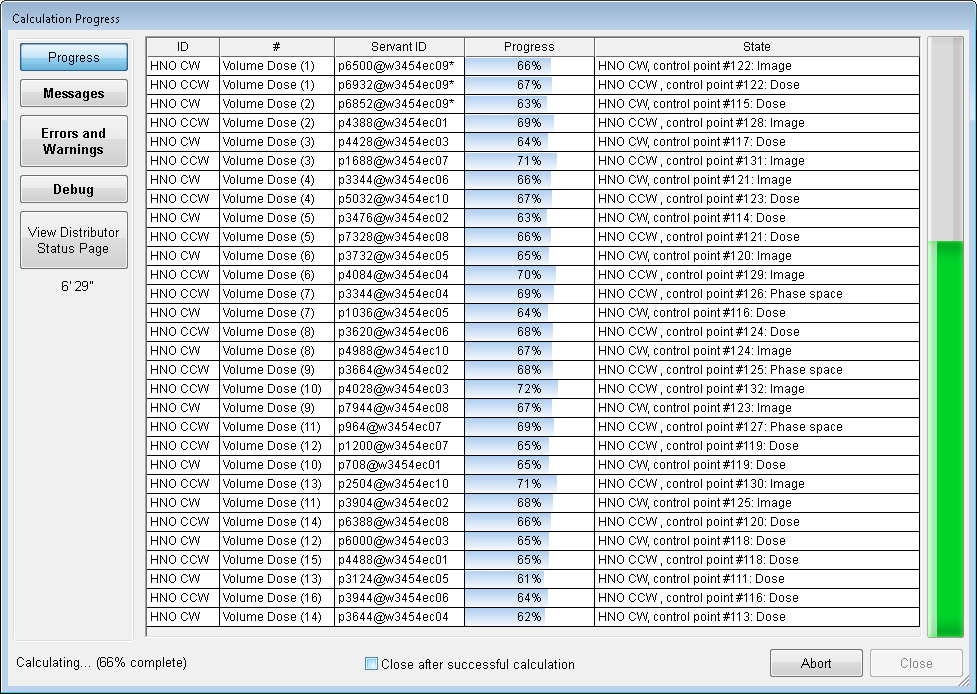
All versions in this experiment were 10.0.28. Our Distributed Calculation Framework (DCF), which takes care of dose calculation, currently consists of 10 Eclipse workstations, named w3454ec01 to w3454ec10, with a total number of 88 CPUs and 216 GB RAM:

The operating system is either WindowsXP-64bit or Windows7-64bit. Here is s screenshot of the Task manager during a typical AXB calculation of two 360° arcs and large fields, at 90% progress. The AcurosServant.exe uses about 5 GB of RAM.
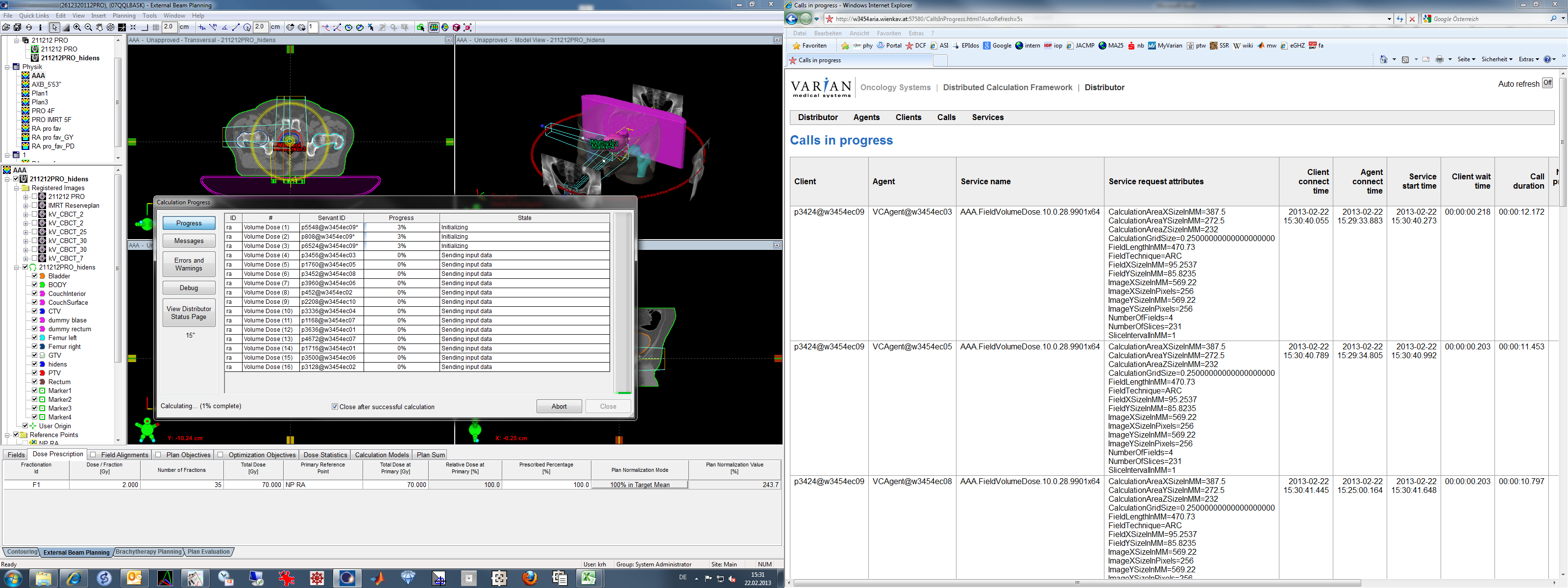
During the tests on Eclipse workstation w3454ec09, the DCF load was closely monitored, to make sure that at the time at the beginning and during dose calculation only w3454ec09 was present as Client (first column) and did not serve as Agent (second column), which means that no other calculation on the network used the local resources. This was accomplished by using the DCF web interface on port 57580 of the ARIA server and the Auto Refresh function:{kind=link}
{kind=link}
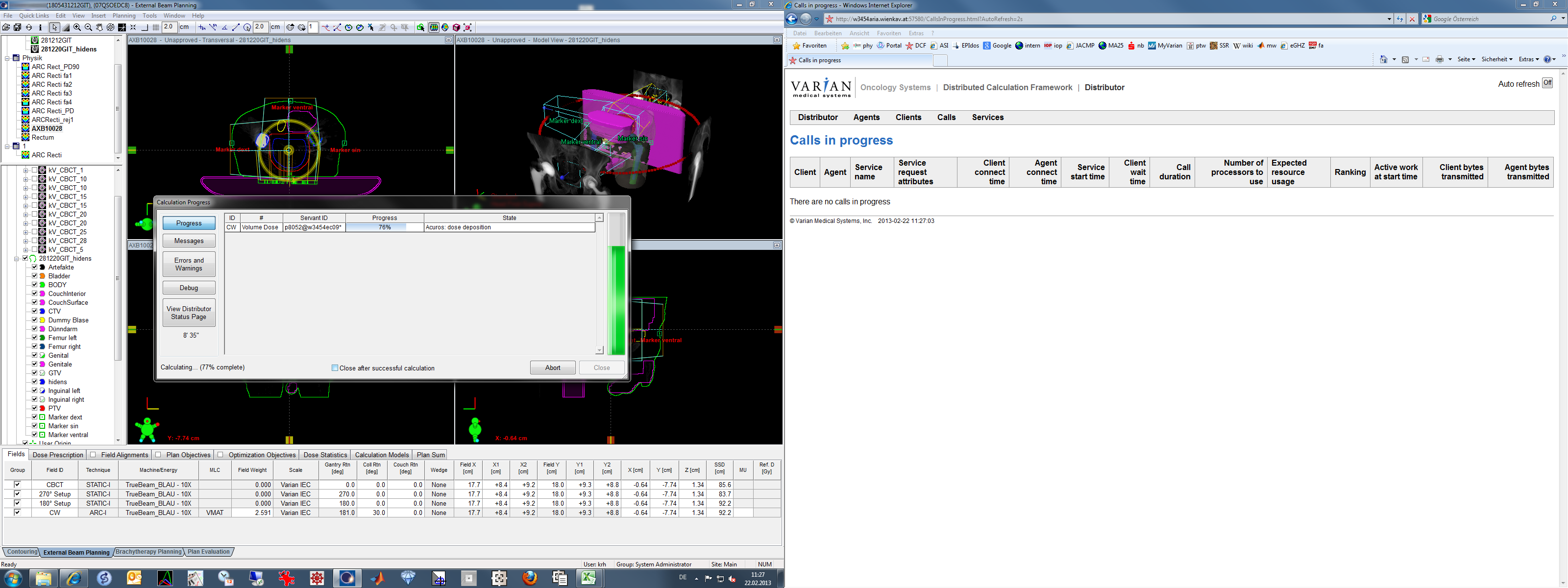
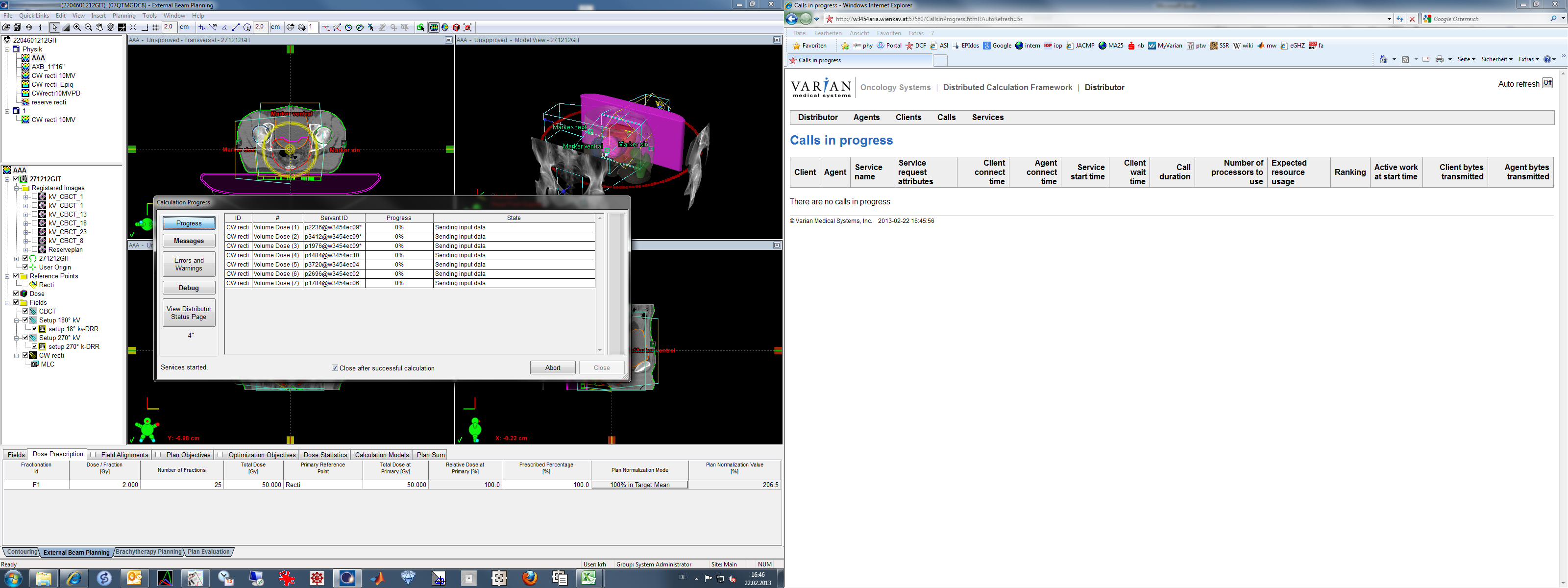
("No calls in progress", the desired situation in the case of AXB and AAA)
{kind=link}
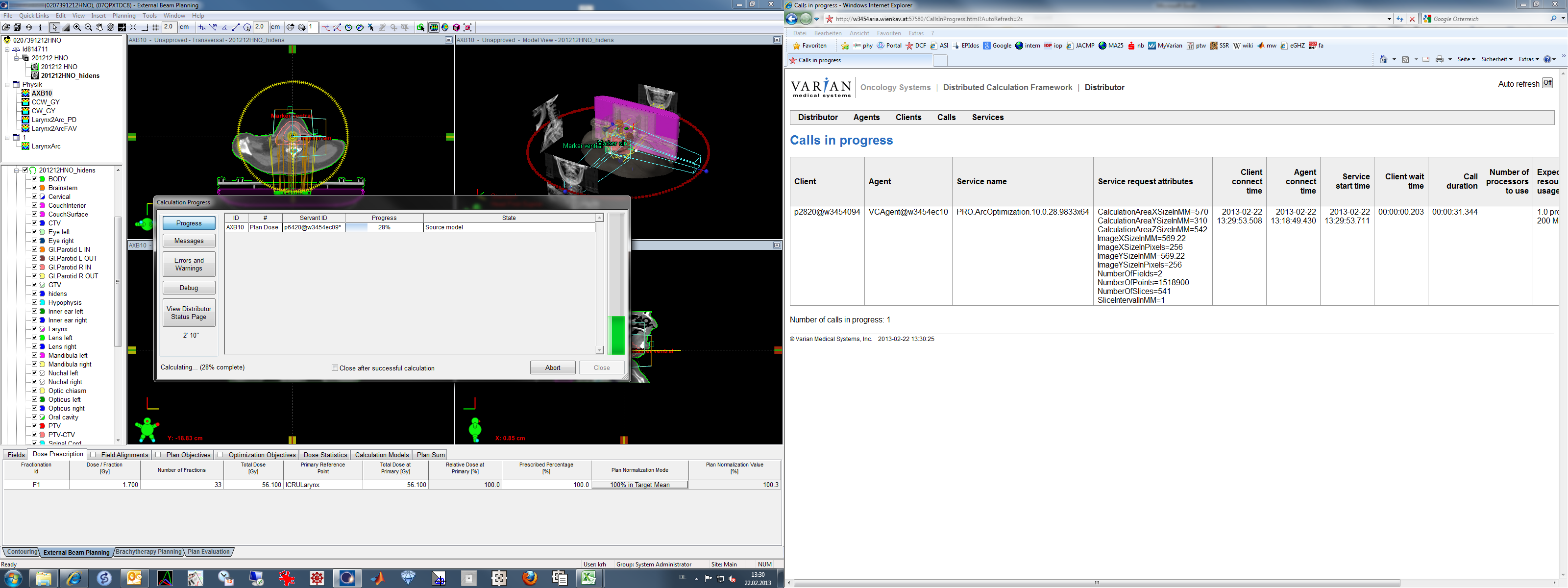
However, in the case of AXB and plan dose, it would be OK if other agents (not the local w3454ec09) are performing jobs for other clients, since this would not compromise the local timing results.
{kind=link}
Calculation Settings
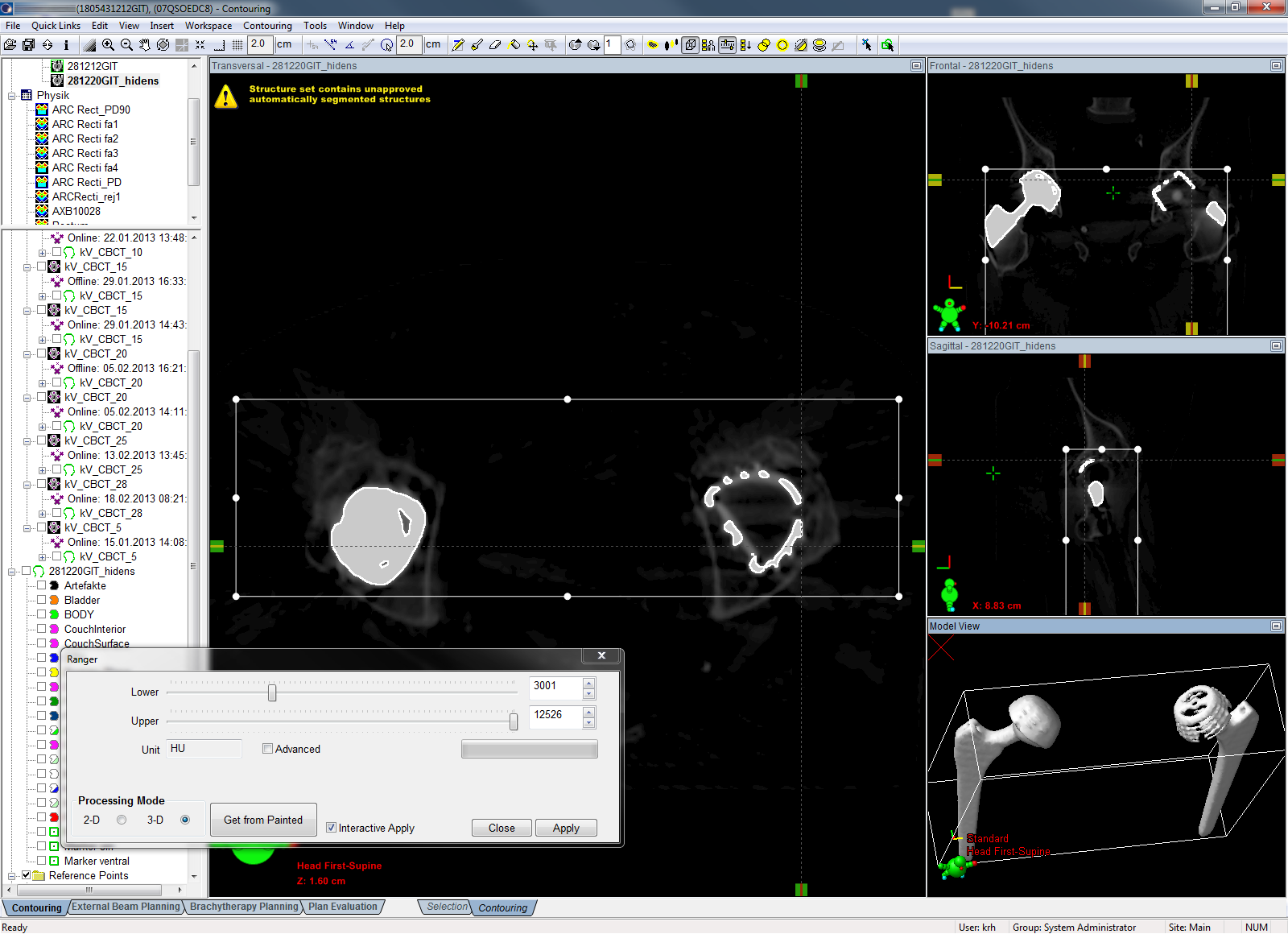
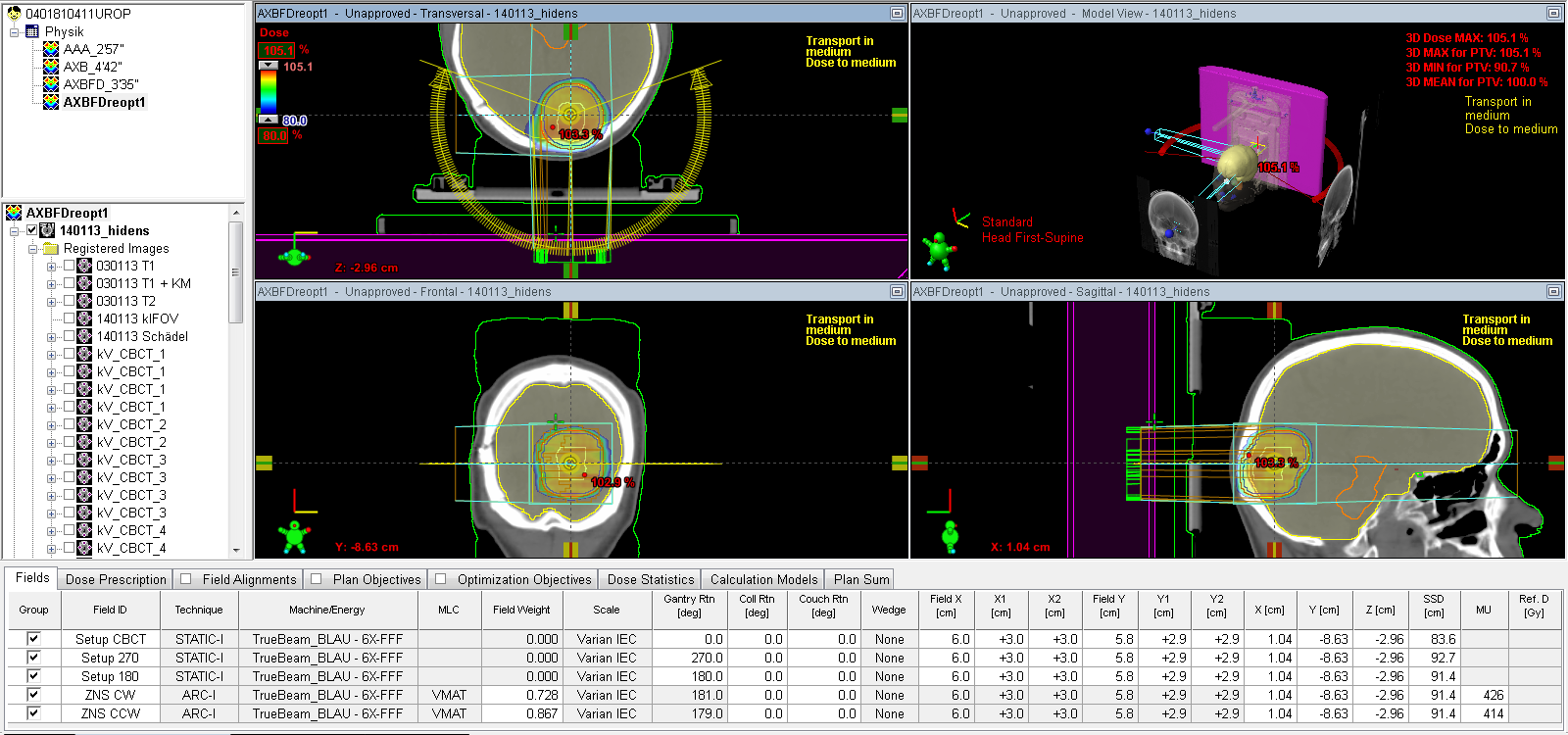
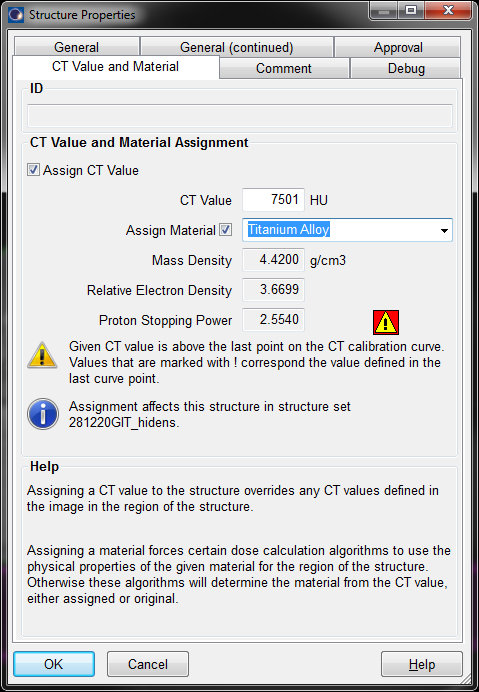
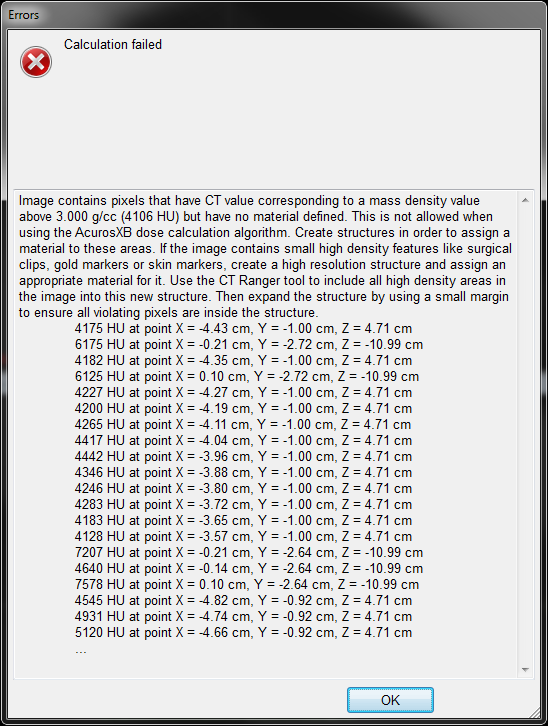
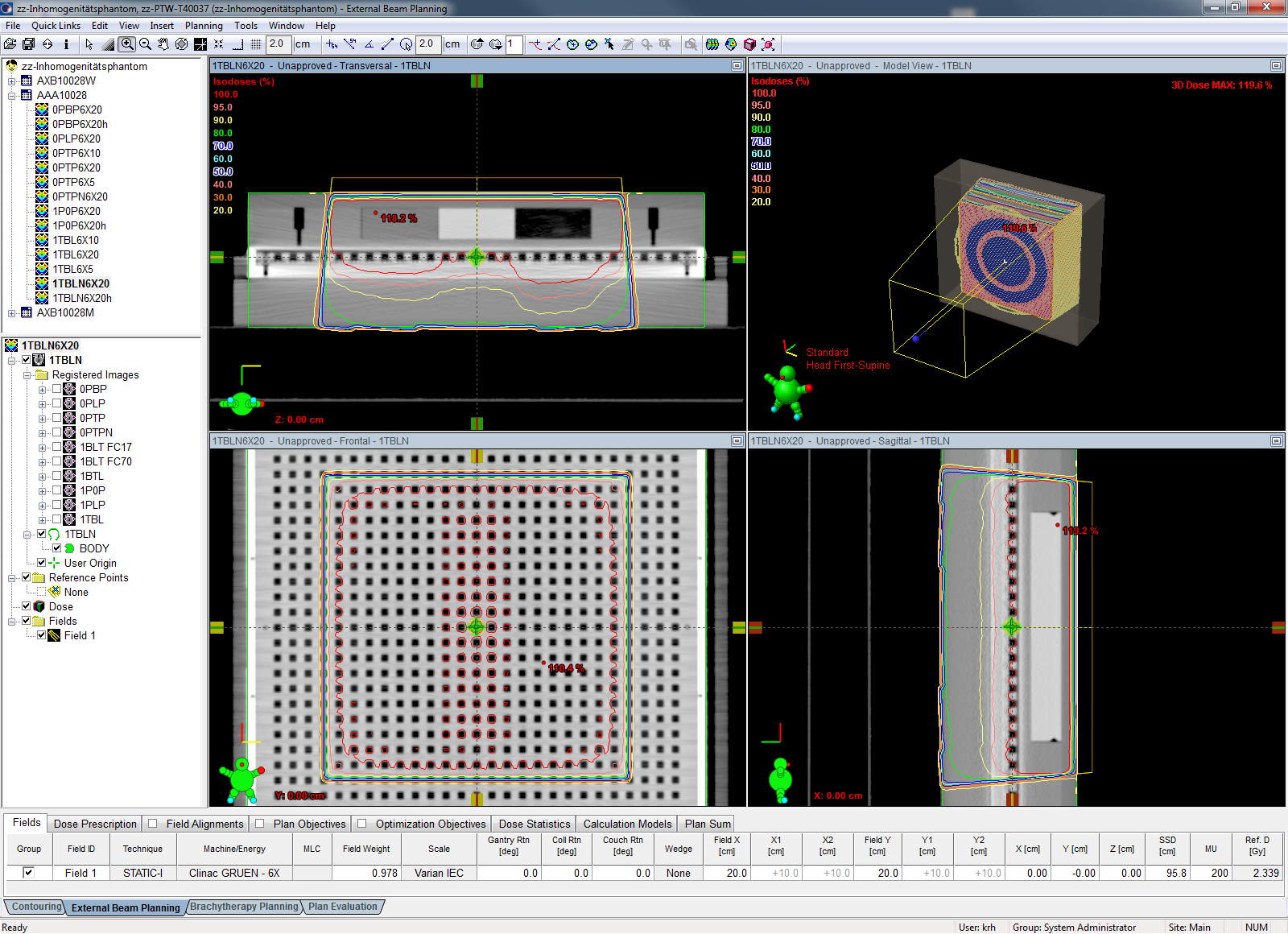
For both AAA and AXB, the calculation grid size (one key parameter for calculation time) was set to 2.5 mm. The calculation defaults for AAA and AXB were used. If the Structure Set contained high density material above 3 g/cm3 (see sidebar) and AXB refused calculation, the Structure Set was duplicated and a dummy high density structure was created which masked the high density voxels. This Structure Set was then used for both AAA and AXB dose calculations.
{kind=link}
{kind=link}
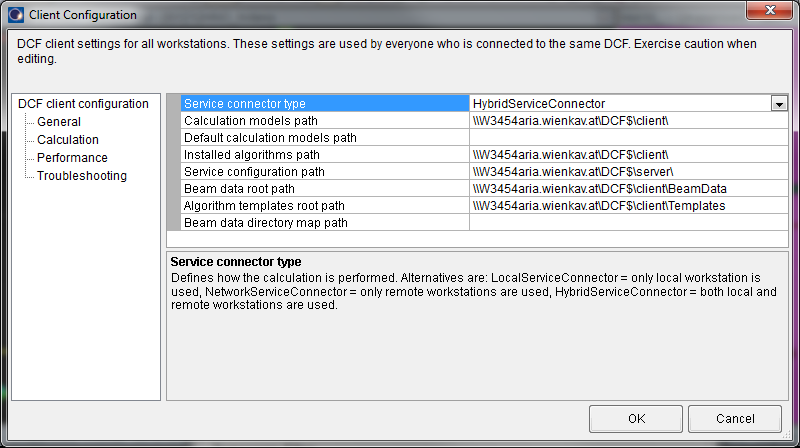
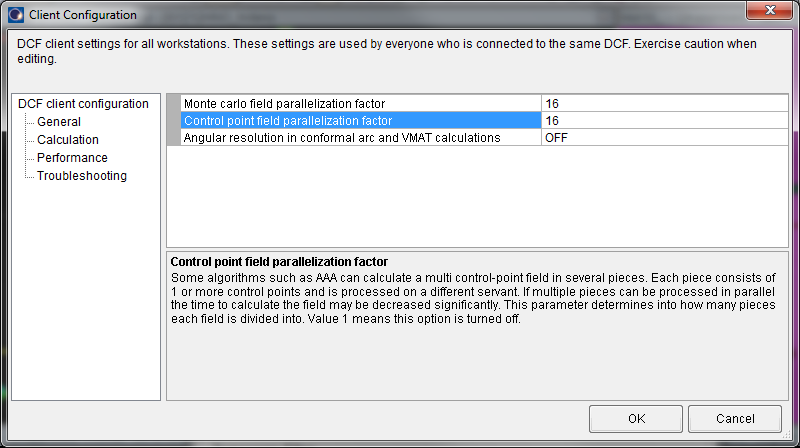
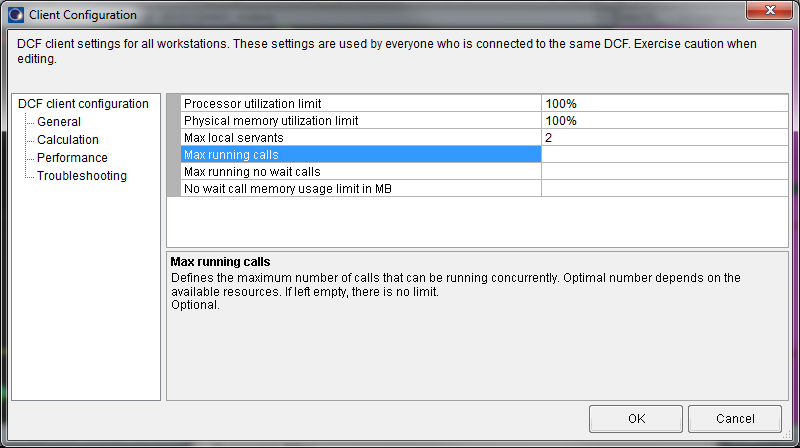
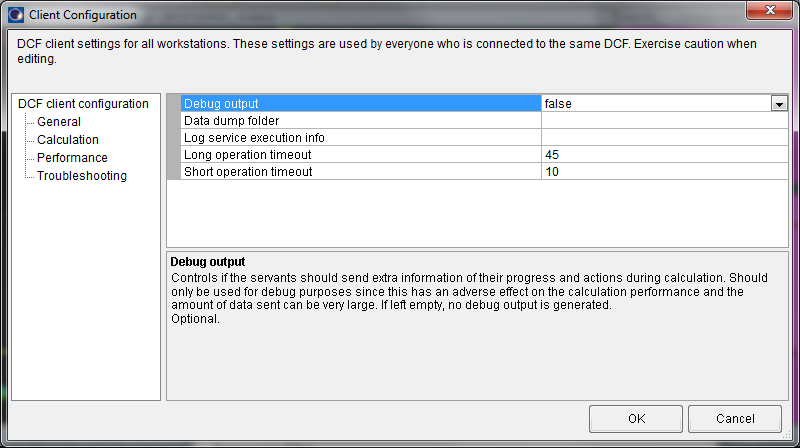
We use global DCF settings with no local overrides. The Service connector type is hybrid, the Control point field parallelization factor is 16, the performance parameters are set to maximum (the Max running calls parameter only affects version 8.1 - 8.9 and has no function here), and debug output is set to false, since this could reduce performance.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patients
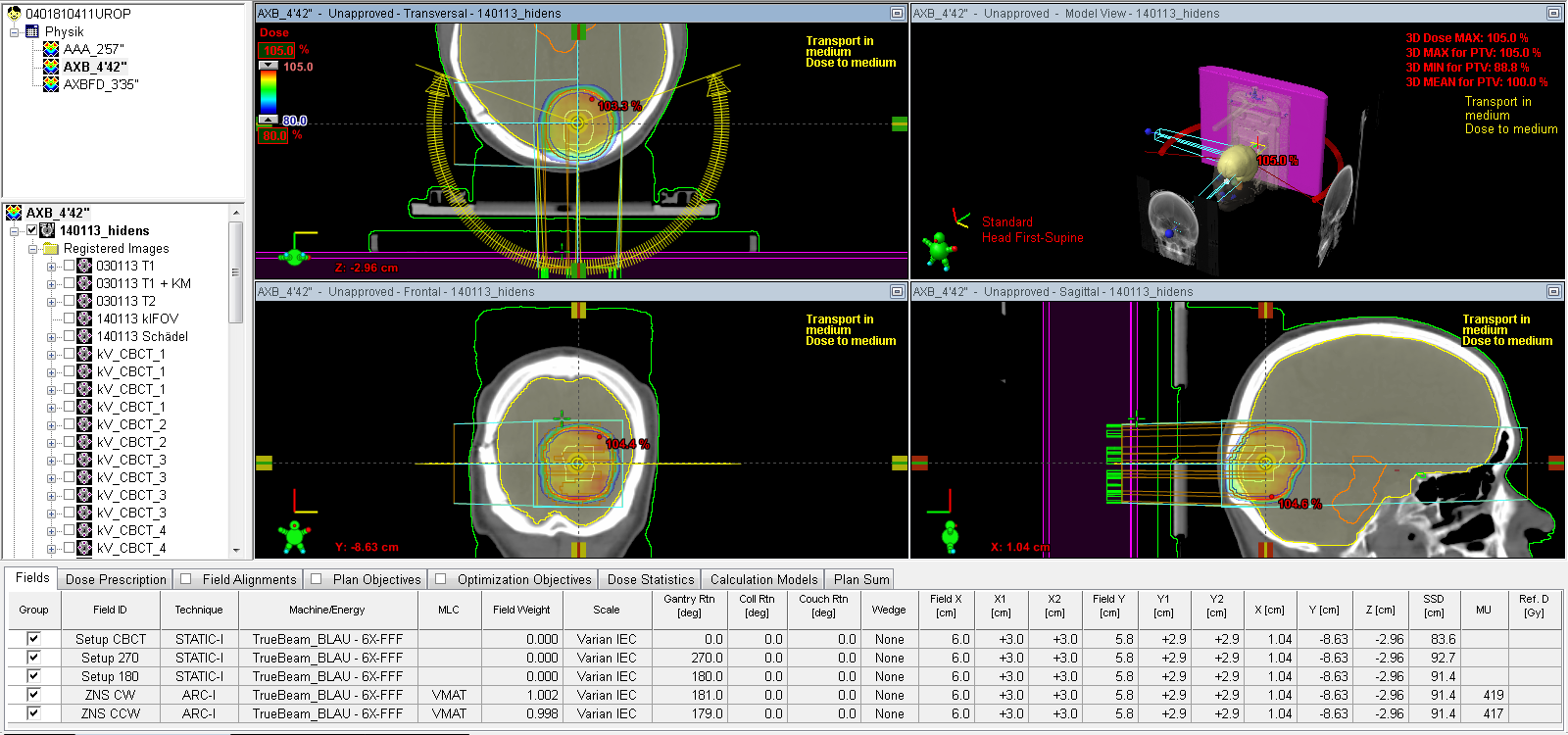
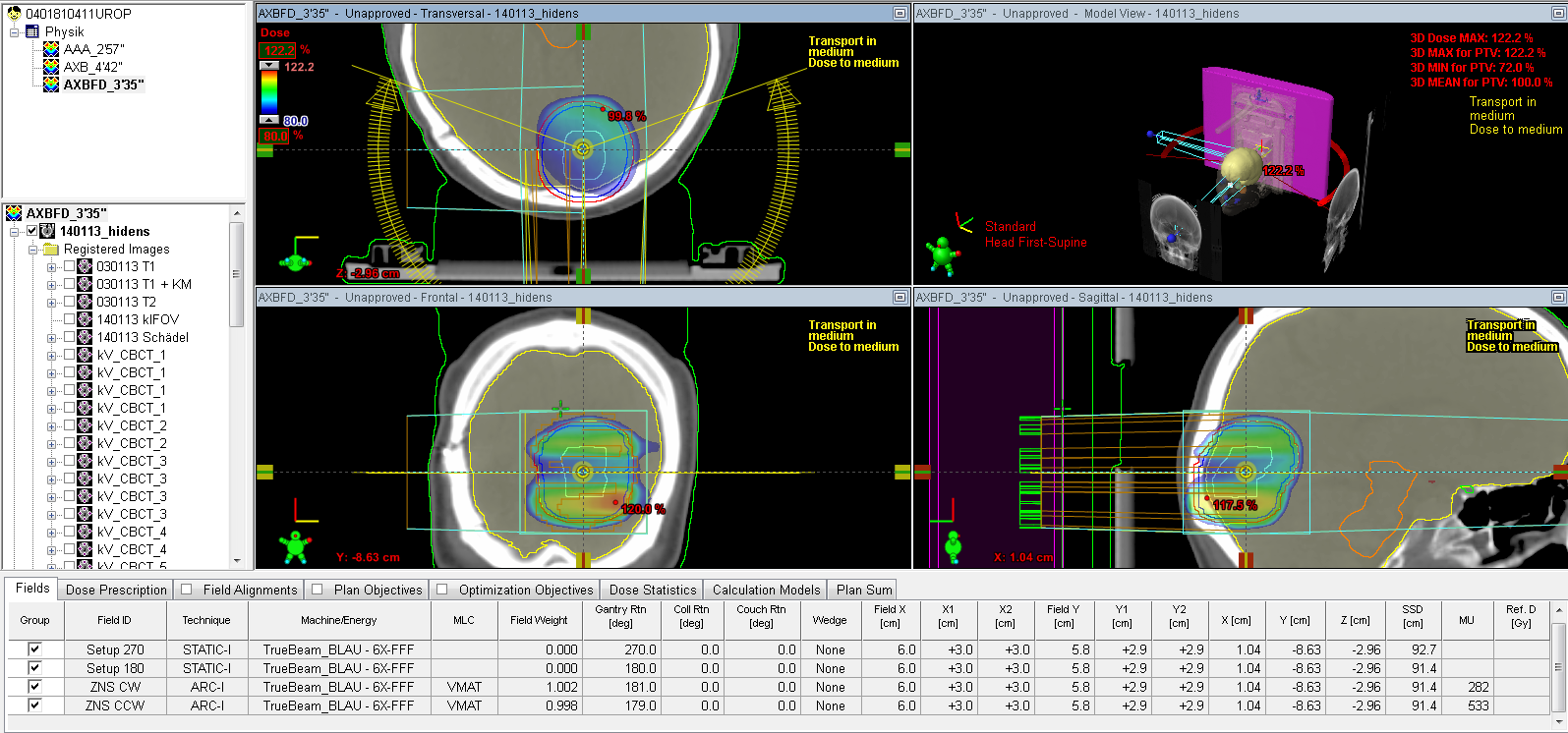
The first 20 RapidArc patients of 2013 were recalculated both with AAA and AXB in a separate "Physics" course. Since the clinical plan was always AAA, we made a copy of the plan, pasted it into the Physics course and changed the algorithm to AXB. This cleared dose. The calculated AXB plan was again copied, pasted, and algorithm was changed back to AAA, and recalculated. We think that this removed any effects of memory cache which might distort the results.
After calculation, the time was entered as part of the plan name. Several plans were calculated twice, to check the reproducibility of the timing. Timing differences were always within 10%.
The following table lists patient information about the treatment sites, the number of planning CT slices, slice thickness (in mm), whether a high density structure had to be created or not, the combined volume (in cm3) of all targets in the plan, the number of arcs, and the total arc angle:
| Pat # | Location | Slices | Thickness | Hidens? | PTV [cm3] | Arcs | Total ° |
|---|---|---|---|---|---|---|---|
| 1 | Rectum | 295 | 1 | yes | 1188 | 1 | 360 |
| 2 | Abdomen | 171 | 2 | no | 141 | 1 | 210 |
| 3 | HeadNeck | 261 | 1 | yes | 453 | 2 | 720 |
| 4 | Prostate | 231 | 1 | yes | 116 | 1 | 360 |
| 5 | Rectum | 248 | 1 | no | 1048 | 1 | 360 |
| 6 | Rectum | 251 | 1 | no | 1249 | 1 | 360 |
| 7 | Rectum | 375 | 1 | no | 1572 | 2 | 720 |
| 8 | Prostate | 340 | 1 | no | 620 | 1 | 350 |
| 9 | HeadNeck | 297 | 1 | yes | 362 | 2 | 720 |
| 10 | Prostate | 233 | 1 | yes | 250 | 1 | 360 |
| 11 | Head | 413 | 1 | yes | 63 | 2 | 220 |
| 12 | HeadNeck | 297 | 1 | yes | 450 | 2 | 720 |
| 13 | HeadNeck | 377 | 1 | yes | 502 | 2 | 720 |
| 14 | Abdomen | 427 | 1 | yes | 377 | 1 | 360 |
| 15 | Lung | 409 | 1 | yes | 131 | 2 | 385 |
| 16 | HeadNeck | 347 | 1 | yes | 123 | 2 | 360 |
| 17 | HeadNeck | 267 | 1 | no | 74 | 1 | 180 |
| 18 | Anal | 342 | 1 | no | 2364 | 4 | 720 |
| 19 | Prostate | 282 | 1 | yes | 296 | 1 | 360 |
| 20 | HeadNeck | 345 | 1 | yes | 610 | 2 | 720 |
Results
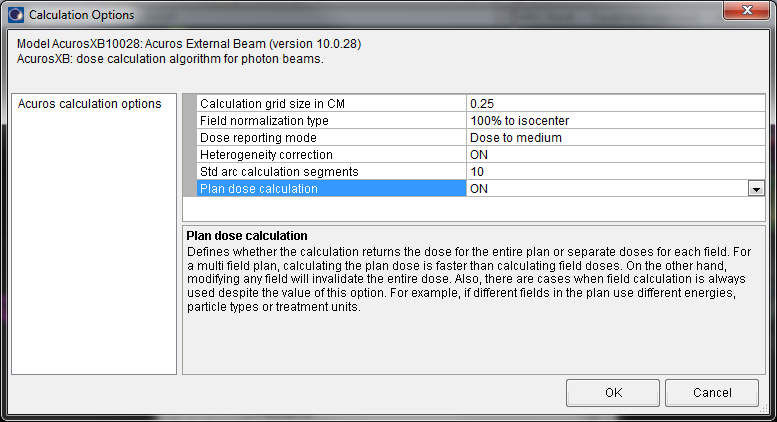
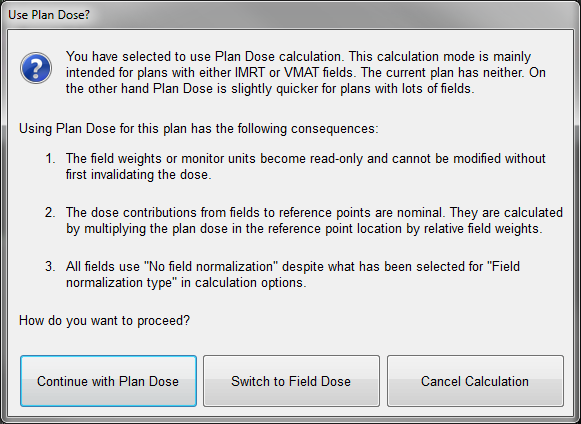
When plan dose was used, the AXB calculations always took longer than the AAA calculations, by a "prolongation factor" of 2.4 ± 0.7 (columns 3 and 4 in the following table).
For field dose calculation, the picture changed (columns 5 and 6). If a plan contained more than one arc, calculation time went down, and so did the prolongation factor (1.2 ± 0.2 for the 10 plans which had more than one arc). Patient 18 (plan with 4 arcs) was even calculated faster with AXB than with AAA.
| Pat # | AAA [s] | AXB-PD [s] | Factor | AXB-FD [s] | Factor |
|---|---|---|---|---|---|
| 1 | 171 | 710 | 4.2 | 708 | 4.1 |
| 2 | 83 | 194 | 2.3 | - | - |
| 3 | 301 | 620 | 2.1 | 369 | 1.2 |
| 4 | 141 | 353 | 2.5 | - | - |
| 5 | 175 | 552 | 3.2 | - | - |
| 6 | 195 | 676 | 3.5 | - | - |
| 7 | 491 | 1200 | 2.4 | 704 | 1.4 |
| 8 | 211 | 510 | 2.4 | - | - |
| 9 | 382 | 739 | 1.9 | 422 | 1.1 |
| 10 | 139 | 408 | 2.9 | - | - |
| 11 | 177 | 282 | 1.6 | 215 | 1.2 |
| 12 | 363 | 779 | 2.1 | 434 | 1.2 |
| 13 | 436 | 843 | 1.9 | 530 | 1.2 |
| 14 | 182 | 376 | 2.1 | - | - |
| 15 | 190 | 301 | 1.6 | 193 | 1.0 |
| 16 | 184 | 394 | 2.1 | 235 | 1.3 |
| 17 | 78 | 135 | 1.7 | - | - |
| 18 | 653 | 1477 | 2.3 | 548 | 0.8 |
| 19 | 167 | 485 | 2.9 | - | - |
| 20 | 481 | 1044 | 2.2 | 601 | 1.2 |
Except for the first patient, we only recalculated those plans in field dose mode which contained more than one arc: for single arc plans, plan dose mode and field dose mode are the same.
Discussion
For the first 20 patients treated with RapidArc at KFJ, in plan dose mode the "ultrafast" AcurosXB10 always calculated slower than AAA10, by a factor of about 2.4.
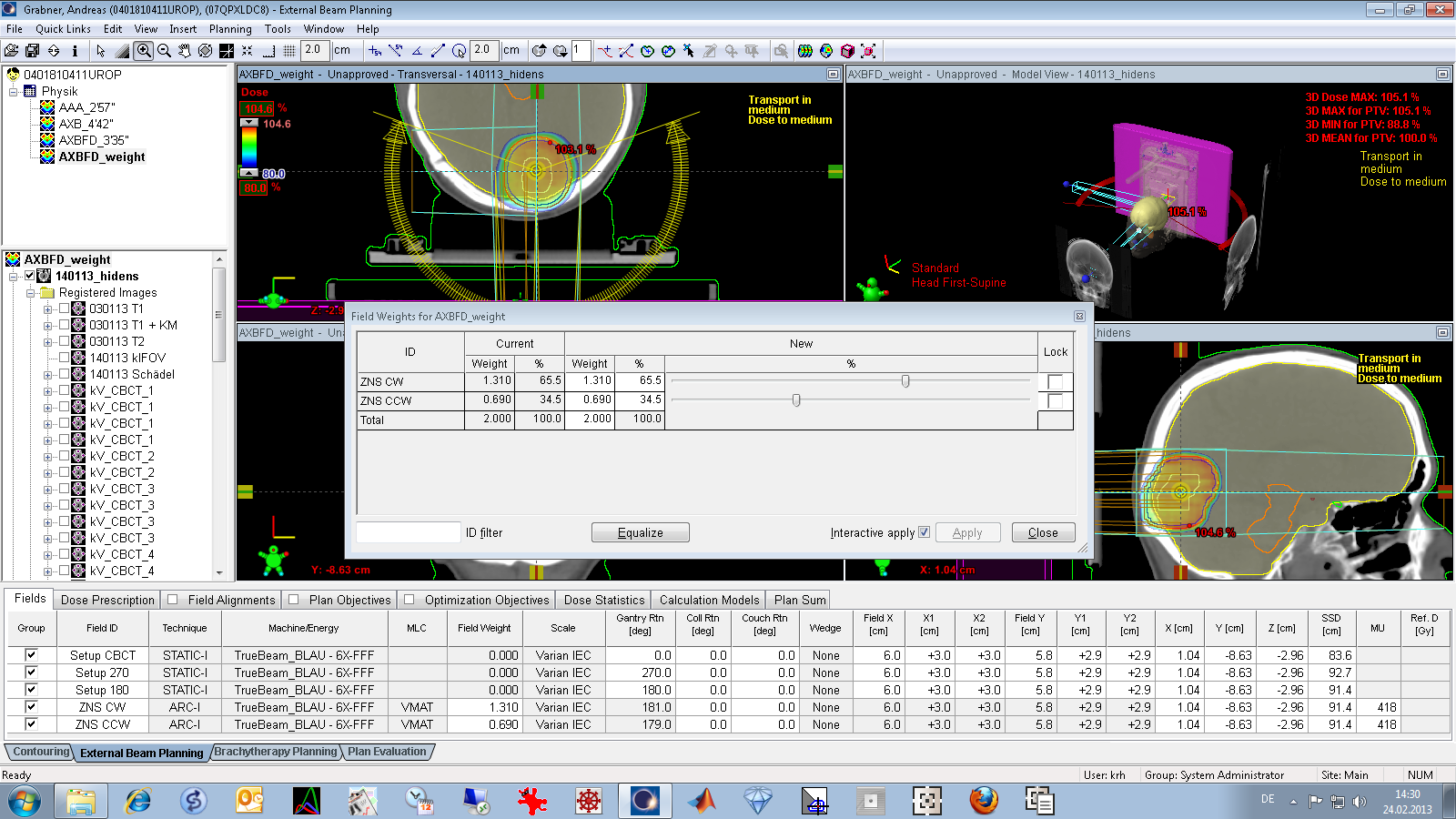
When a plan contains more than one arc, it makes sense to use AXB field dose calculation. One arc is always calculated locally, no matter what the dose calculation mode is. The other arcs take use of the DCF, so the overall calculation time will go down significantly.
On a decent DCF (DCF = Decent Calculation Framework) with 10 Eclipse workstations, the parallelization feature works in favor of AAA: AAA can send Control points to the DCF, Acuros can only send full arcs (or single fields). In other words, in our case the DCF somehow is the competitor of Acuros. However, if one looks at the timing "per workstation", Acuros is really fast, at least for RapidArc plans. However, if only a single static 20x20 cm field is calculated, it takes 11" with AAA, but 227" with AXB, which is over 20 times longer ...
{kind=link}
{kind=link}