
{kind=link}
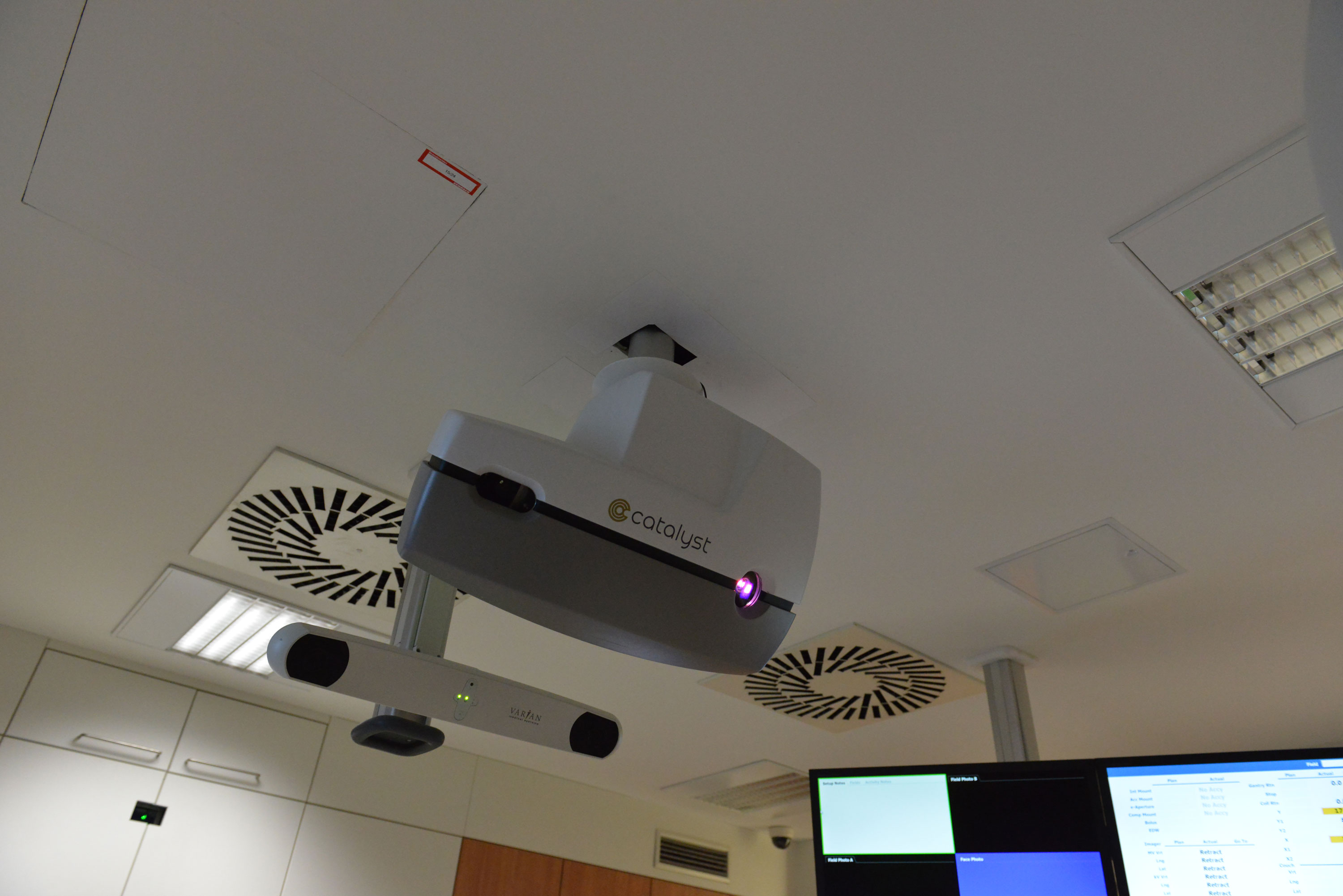
Catalyst is a surface scanner/backprojection system which helps the therapists to position the patient before the treatment:
It is also used to monitor patient movement during treatment. If a gating license is purchased, it will be possible in the future to perform gated treatments on the TrueBeam1.
Patient Setup
We briefly list the steps of a typical breast setup (two tangential fields) at our institute using Catalyst HD:
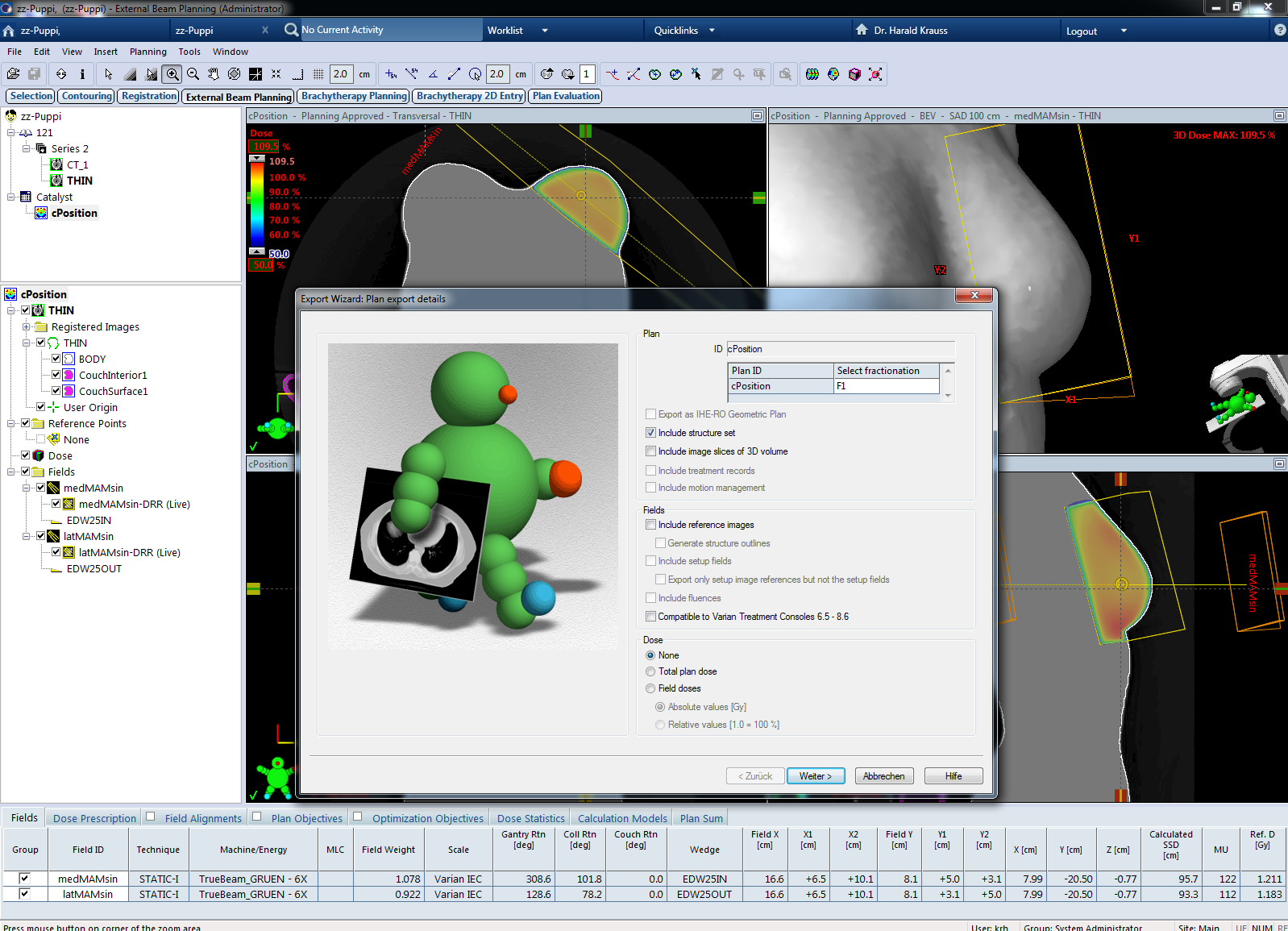
- The treatment plan is exported from Eclipse including the structure set. The structure set contains the BODY structure, which will serve as reference during patient setup.
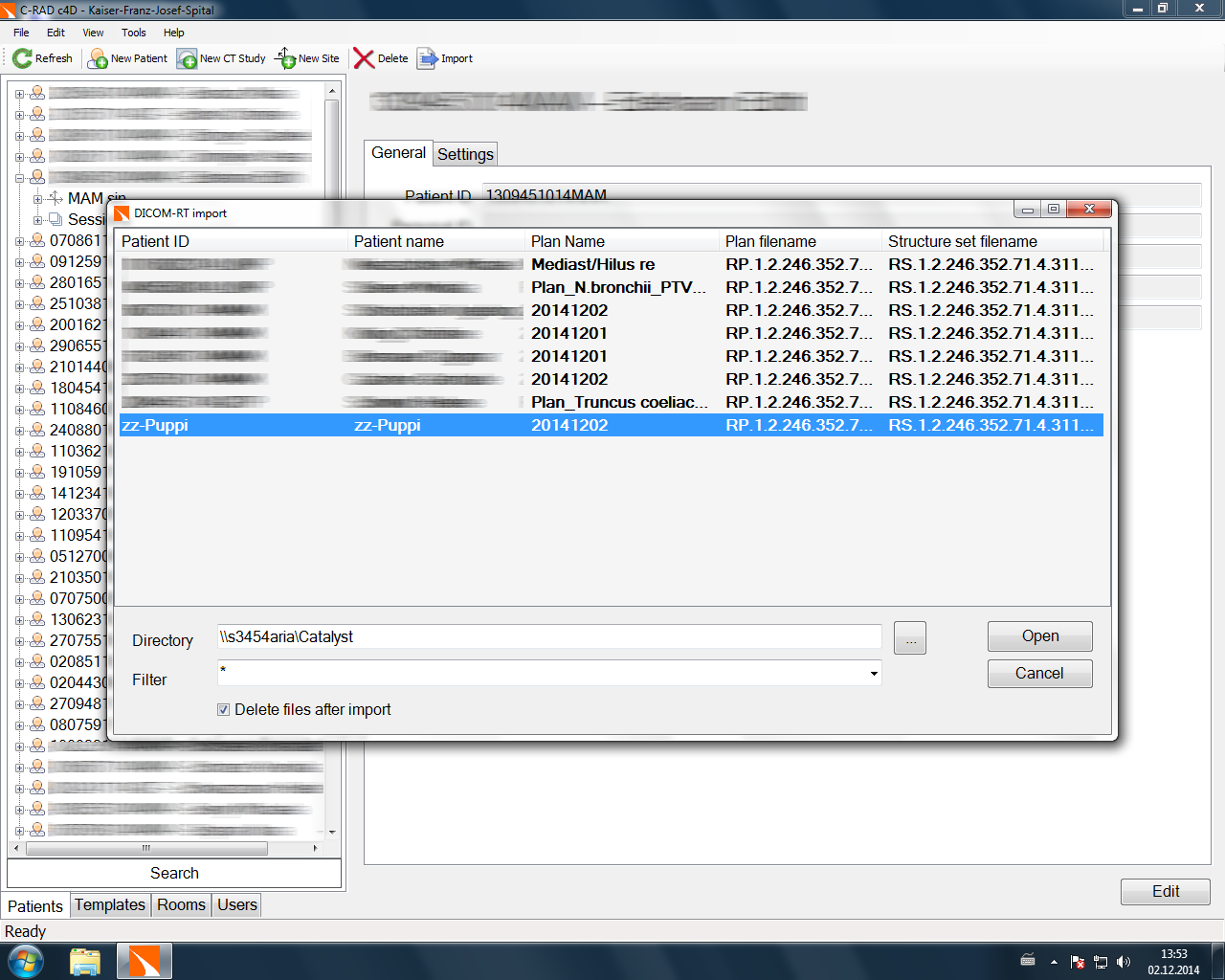
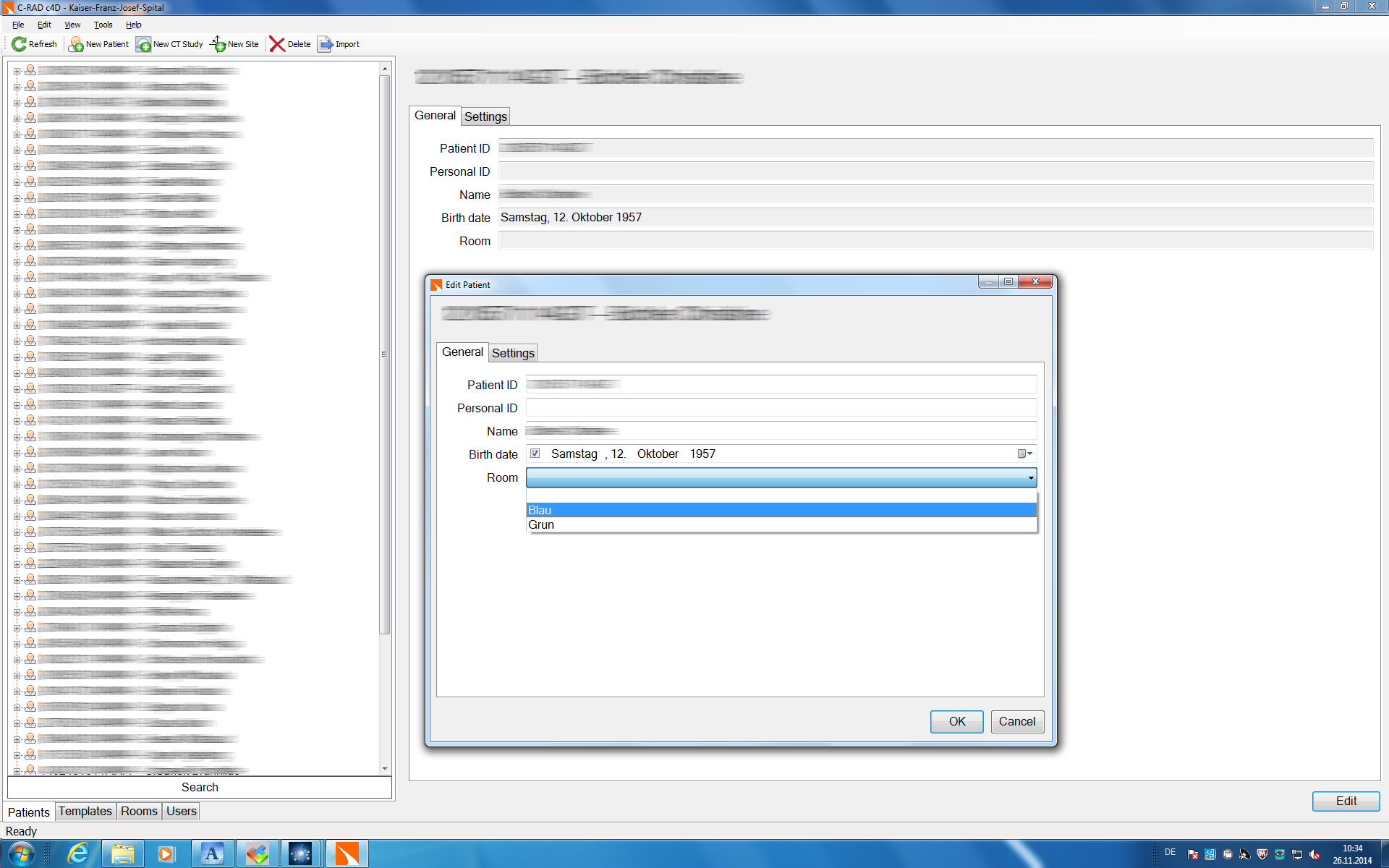
- On a Catalyst workstation (either the online workstation located in the TrueBeam control room or an off-line workstation), the plan is imported. If this is done off-line, the treatment room has to be specified too.
- During the import process (or later), a user-defined template can be applied. The template contains a set of settings which are optimized for the treatment site (one could also implement settings for different skin colors, etc.).
- Under the tab cPosition (the mode which will be used for patient positioning), the Scan Volume can be restricted to the volume which shall be used for isocenter calculation:
{kind=link}
{kind=link}
{kind=link}
{kind=link}

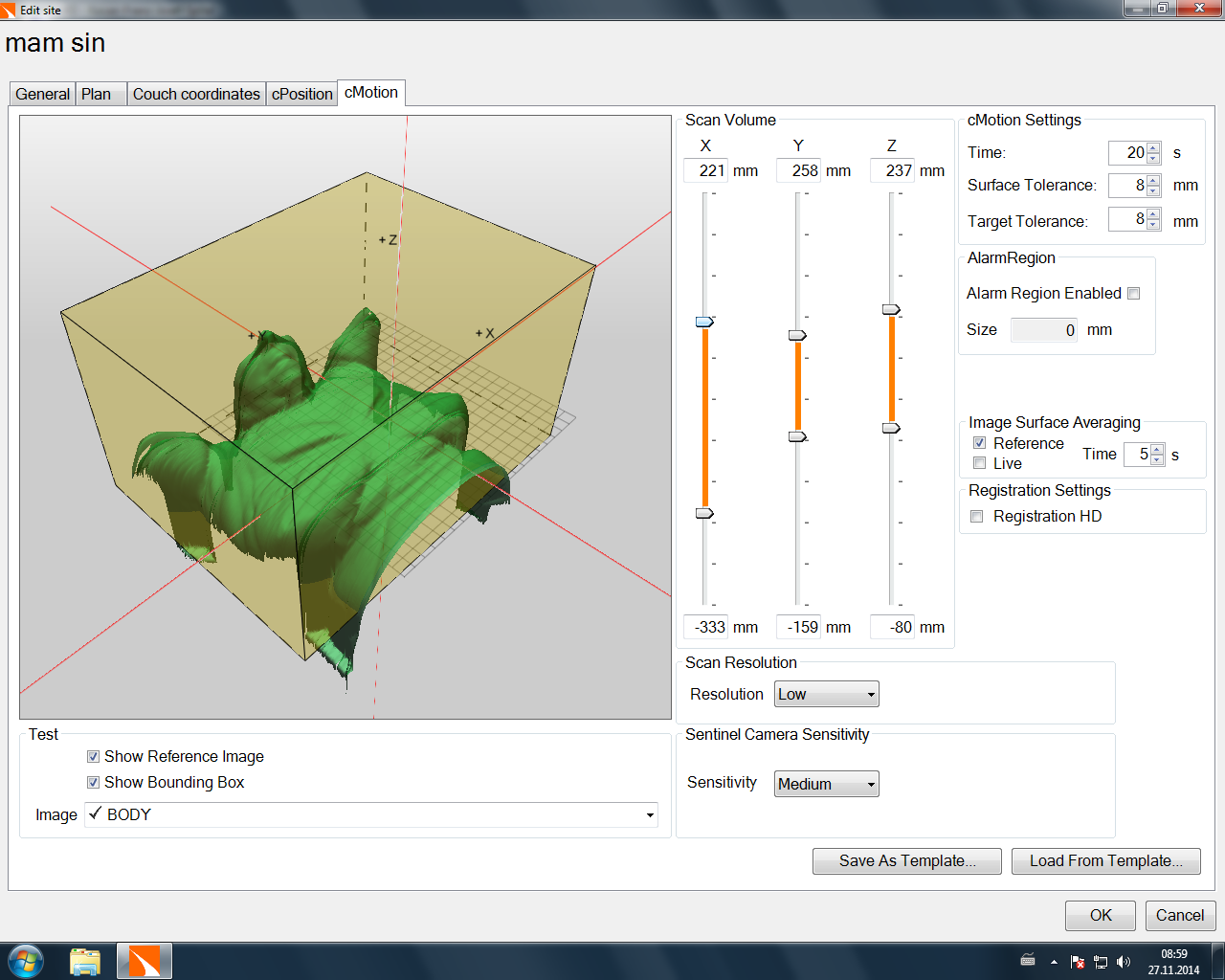
- The settings for the cMotion mode (the supervision mode which is used to monitor patient motion during treatment) can be set independently.
- Now the patient can be loaded on the online Catalyst workstation in Clinical Mode, first with cPosition.
- The patient is positioned on the couch.
- If it is a 1st-day-setup, first isocenter is established according to plan parameters. Then Catalyst is used2 to "fine-tune" patient position or move parts of the body as necessary, until the residual isocenter error as displayed on the Catalyst screen is acceptable (our internal action level is 3 mm).
- From the 2nd day on, first the isocenter is established by aligning skin marks (which had been applied in the 1st treatment session) with the room lasers, fine-tuning is again with Catalyst.
- The therapist in the treatment room switches to the treatment or monitoring mode (cMotion), in order to detect any patient movement which occurs from now on, and leaves the treatment room.
- If it is a 1st-day-setup, TrueBeam imaging is used to improve the isocenter position by performing the sequence of kV-kV-imaging, matching, and applying couch shifts.
- From the 2nd day on, only one beam-before-MV-image is taken for one of the tangential breast fields, to verify the Catalyst result.
- Treatment is started.
{kind=link}
cPosition
During patient setup, cPosition permanently calculates the actual isocenter after performing a non-rigid registration with the reference surface and displays the necessary couch shifts on the in-room monitor in near-real-time.
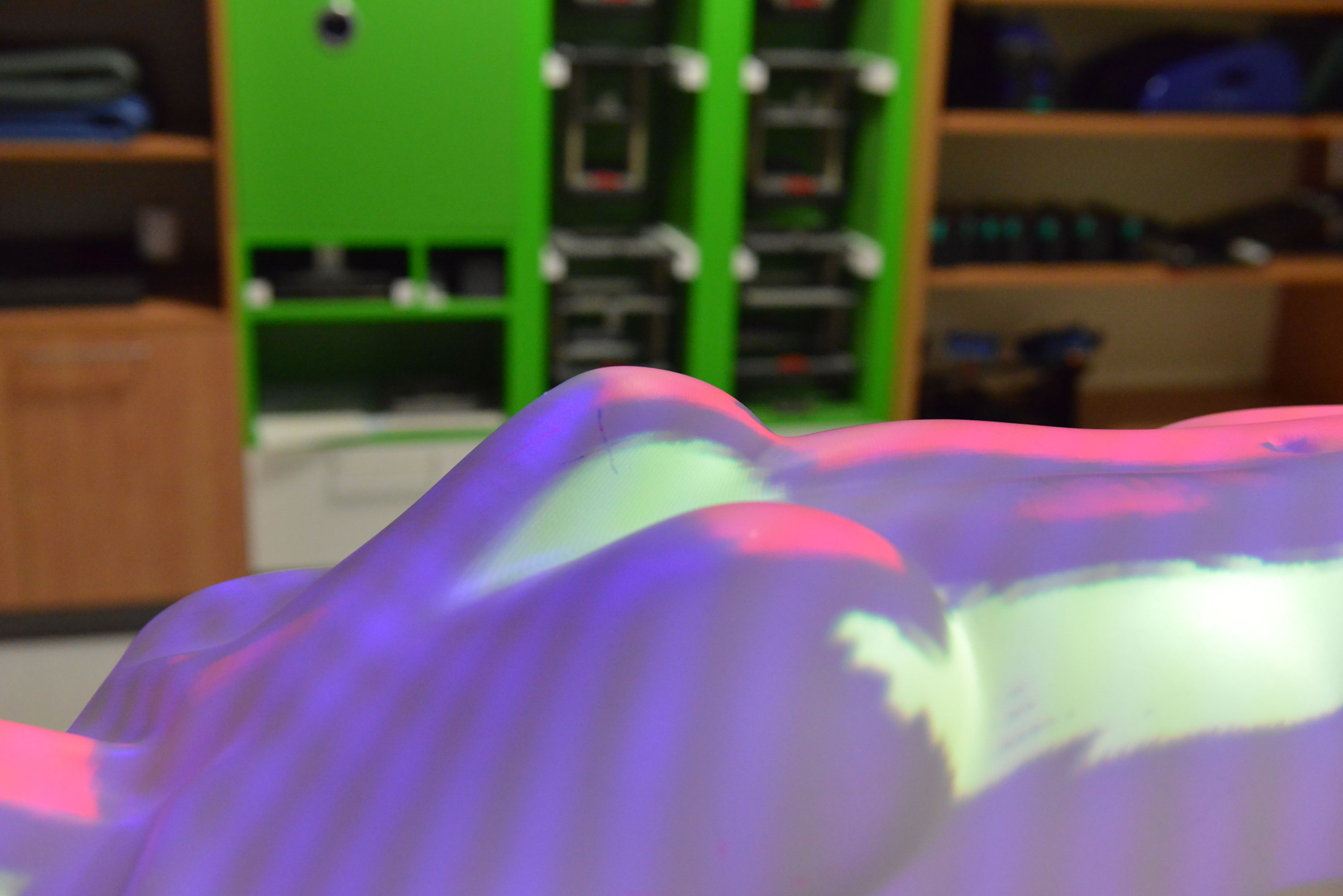
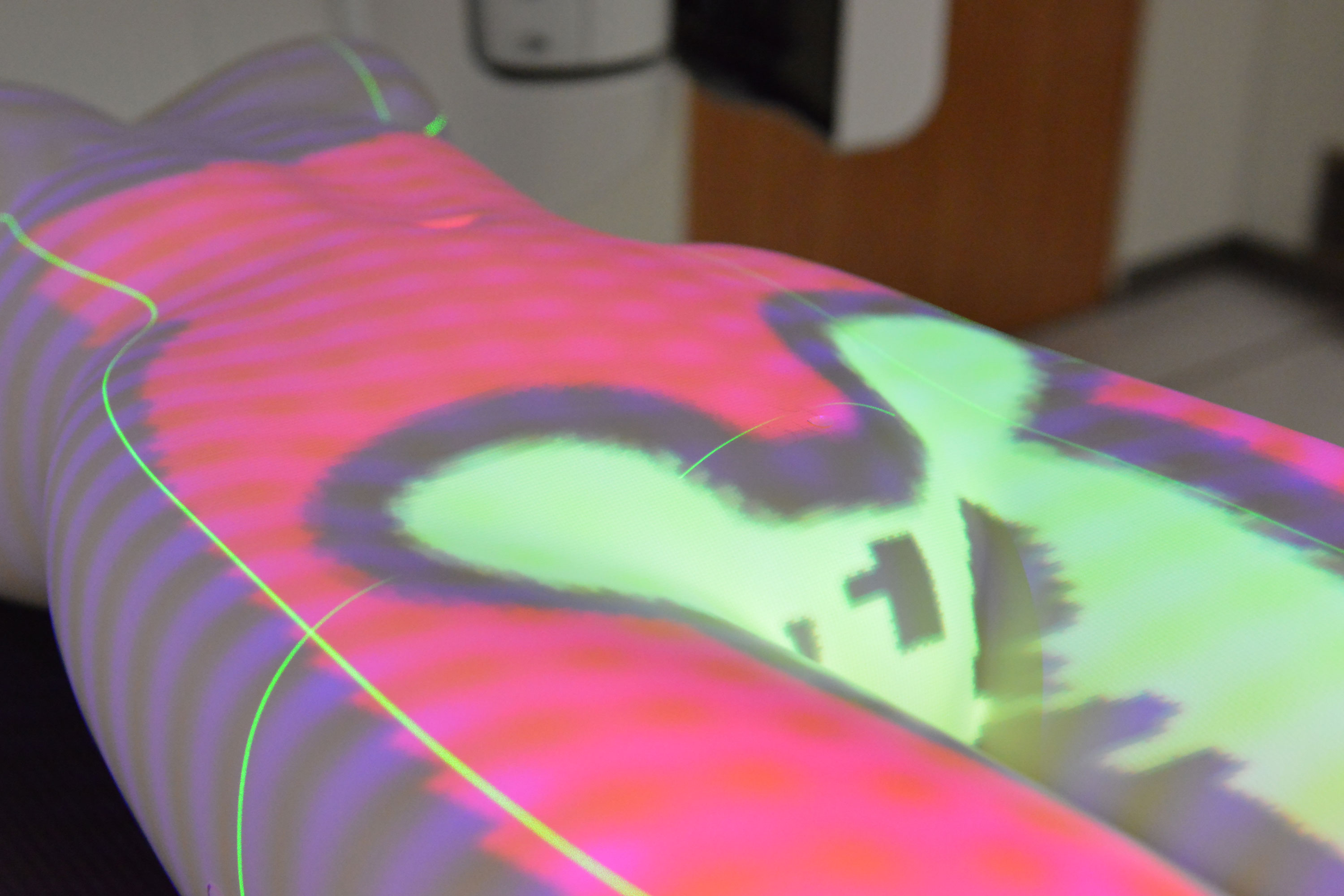
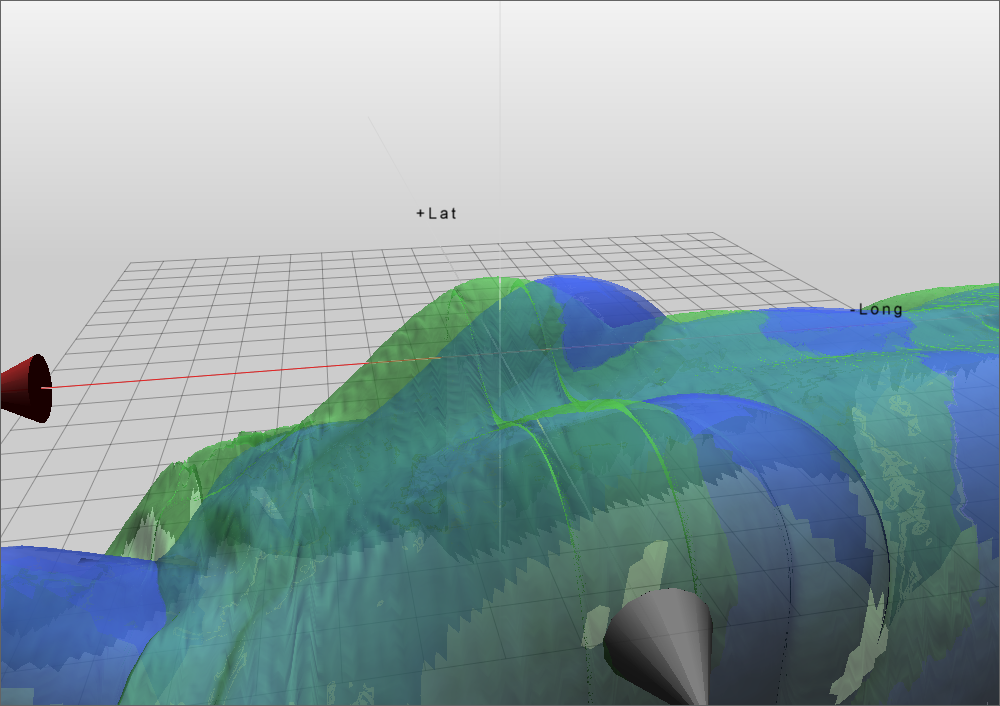
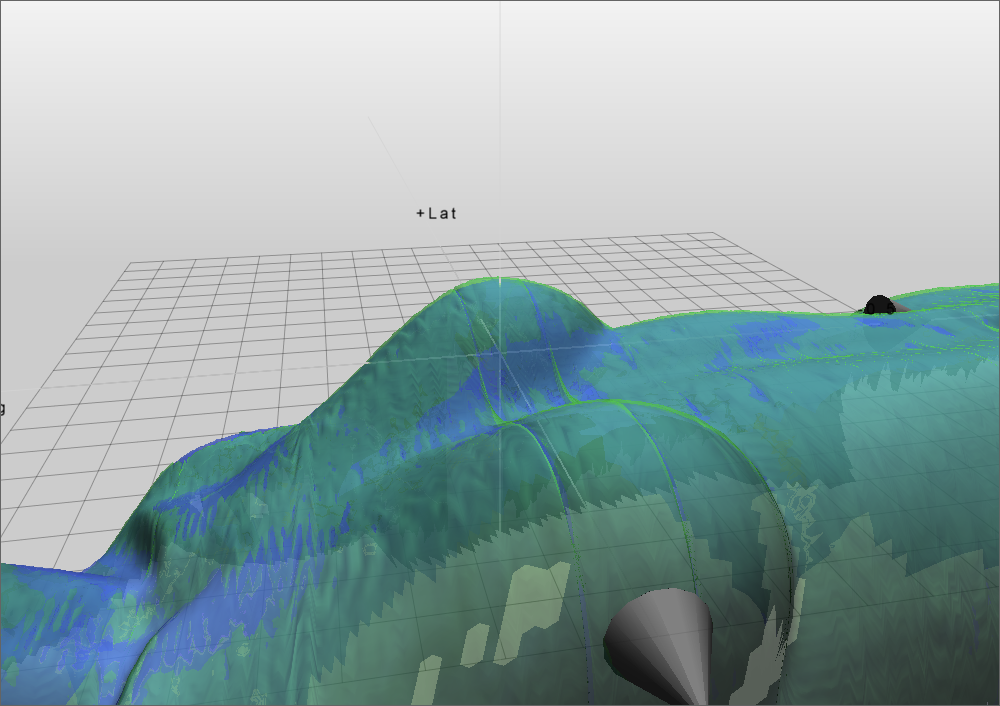
Since the body is non-rigid, this information (lat, long, vert, rot, roll, pitch) is not always sufficient to achieve accurate patient positioning. Therefore, a distance color map can be projected on the patient's surface, which gives information about which part of the body should be moved in which direction (up or down). The following video shows the color coding. Parts of the body which are too high (above ground) are in red, parts which are too low are in yellow.
cMotion
Once the patient position is acceptable after using cPosition, motion monitoring is started by switching to the cMotion module. A session reference image is captured automatically, which is only valid for the current treatment session. The captured reference surface temporarily replaces the Eclipse body outline, which had served as reference during patient setup. All deltas are zeroed, and tiny movements become visible on the screen, which are relative to this session baseline:

Typically (thinking of a general - not only breast - patient), an IGRT imaging process is performed next, either with kV-kV-imaging or CBCT. The image matching gives couch deltas, which are corrected with the Perfect Pitch couch3. The couch movements also show up on the cMotion graphs. If desired, another reference can be captured before treatment is initiated.
Differences in Settings between cPosition and cMotion
We found that the VOI in cPosition should be as small as necessary, and should only cover the volume which is relevant for isocenter calculation, for two reasons. If too large portions of the arms or the chin are in the scan volume and only their positions deviate from reference, this could distort isocenter calculation, although the deviation of these parts of the body are irrelevant for the accurate positioning of the treated region (thinking of a breast patient). The second reason is performance (speed of isocenter calculation). The smaller the scan region, the faster the calculation.
On the other hand, the VOI in cMotion can be quite large, to detect motions in more parts of the body, which are included when capturing the temporary reference.
Clinical Experiences
If certain rules are respected, Catalyst gives accurate results during patient positioning. We see this during 1st-day-setups, when the isocenter is sometimes established by moving to planned coordinates alone while Catalyst is running, but the information is not taken into account by the therapist. The software then displays some residual isocenter error, and after TrueBeam imaging, we often see that Catalyst "was right" (= the residual isocenter error as displayed by Catalyst was the same as the isocenter error after TrueBeam imaging). In other words, if Catalyst would have been used to position the patient in such a case, the remaining couch shifts after TrueBeam imaging would have been very small.
The isocenter calculation process in cPosition sometimes takes quite long. It is often faster to assess the two surfaces visually, and manually move the couch or body parts accordingly. The visual display is much more responsive and robust. The surfaces are always displayed, even under suboptimal conditions.
{kind=link}
{kind=link}
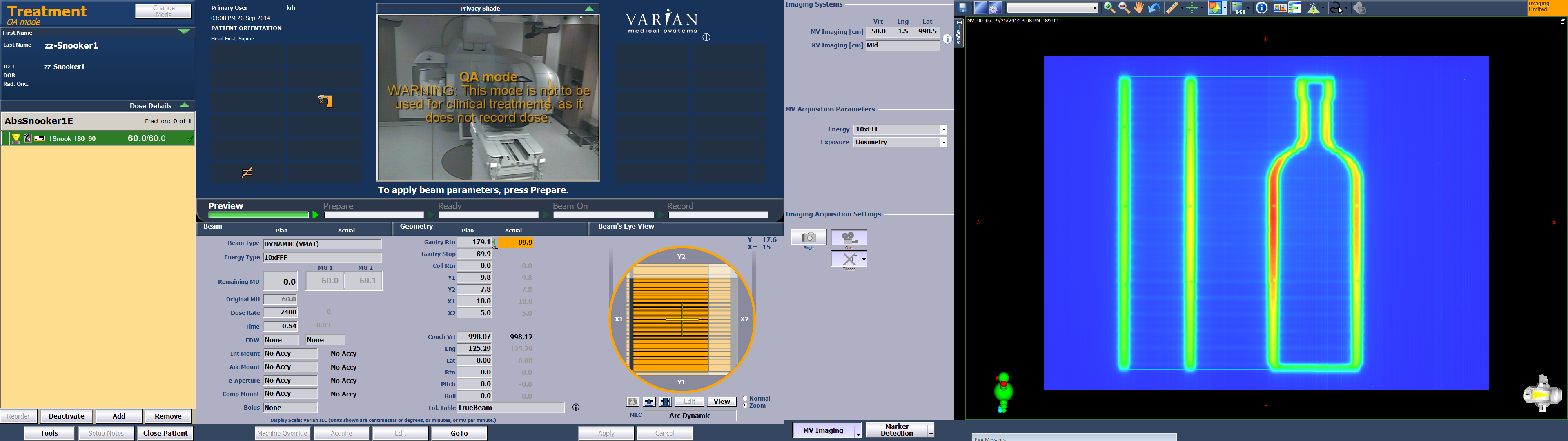
The numerical values for the couch corrections on the other hand are only displayed if the the system decides that the expected accuracy of target calculation is good, otherwise not. In the following video, the patient is moved to target using manual couch control. When target is reached, no more movement occurs (you can hear the "clack" of the couch break at 0:25). However, it takes 30 seconds (0:55), until the system displays the final couch values (we are only interested in the rightmost column with the relative couch corrections):
This can have different reasons (size and quality of input data, lighting conditions etc.). In each individual case, camera settings and other parameter would have to be checked and optimized manually, which is sometimes too time-consuming. Templates have to be checked too, if this occurs too often for a certain target region. In other words, some skill is necessary to use the system optimally. The third video shows how some of the settings are changed:
Some kind of image guidance is performed for every patient, every day. This could either be the single before-image for a breast patient from the 2nd session on, kV-kV-imaging, or CBCT. Each imaging procedure so far confirmed the Catalyst result. On the long run, this will probably reduce the amount of pre-treatment imaging in the future.
It is clear that the results displayed by a surface scanning system will be more accurate if the target is close to the surface, not deep inside the body (and moving, like the prostate). Our main clinical treatment site where Catalyst is used is therefore breast (35% of all patients). Reproducible positioning for breast is more tricky than for treatments in the pelvic region, due to the patient's arms and their degrees of freedom. Other, less frequent sites include the thoracic (lung, oesophagus, ...) and pelvic regions (rectum, ...). About 500 patients have been set up with Catalyst so far.
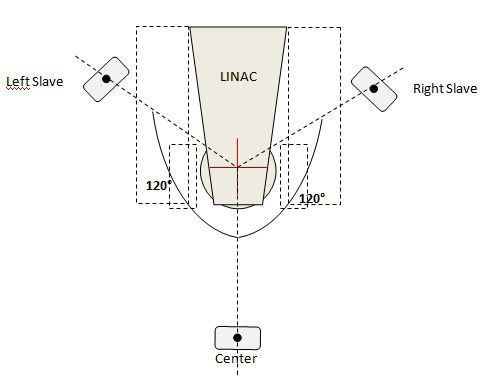
One has to be aware that when the Gantry rotates, the TrueBeam imaging arms (kVS and kVD) block, when extended or even retracted to mid-position, a large part of the camera's scan area. Most of the time the live image then is provided by the 0° scanner alone (which always has an unrestricted view of the patient). The extra (lateral) parts of the rendered surface, which should be provided by the cameras at 120° and 240° often disappear, because either the kVS or the kVD arm blocks the scanner's field of view.
However, when the patient is set up, Gantry is usually at 0°. Then there are free sectors between the imaging arms and the Gantry, where the cameras can look through and see a sufficiently large volume around isocenter.
As already mentioned, currently TrueBeam and Catalyst are not aware of each other. Couch shifts have to be applied manually, using TrueBeam couch controls. Pitch and roll can only be applied after TrueBeam imaging (e.g., Cone beam CT) and matching. This will hopefully be resolved in the future. C-Rad currently develops a TrueBeam interface. Initially (in March 2012), this interface was promised to be available by the end of the year (2012).
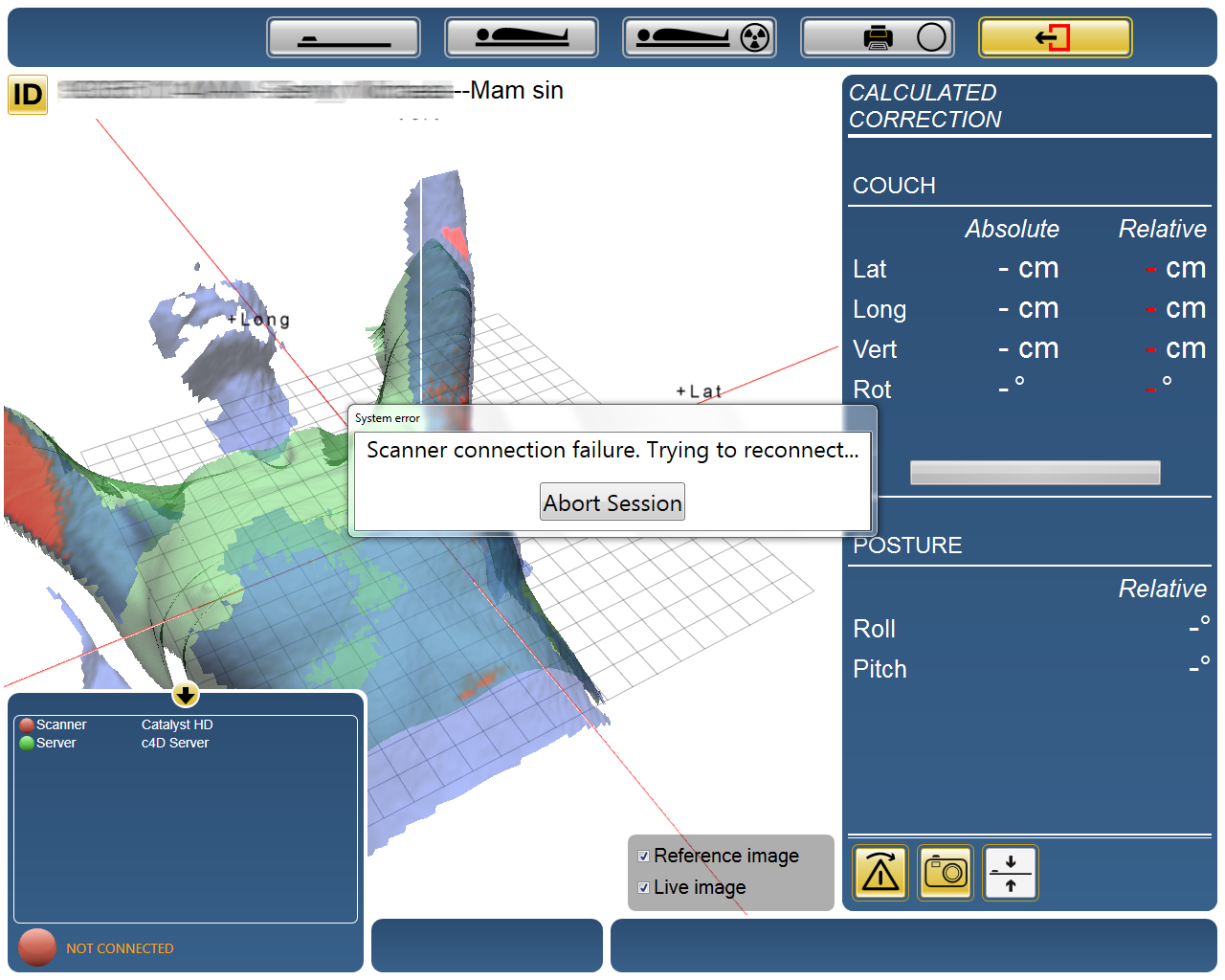
Software stability was less than excellent in the beginning, but has improved with every update. If scanners need to be switched off/on after connection is lost, the Varian LokBar has proved to be of invaluable help to reach the switch of the scanners at 120° and 240°. For the scanner at 0°, it depends on the installation: if there is enough extra space behind the scanner enclosure (which is the case on our TrueBeam "Green"), the LokBar can be used. If the TrueBeam gating camera is too close (like on our TrueBeam "Blue"), it may be necessary to climb on the table to switch the scanner off and on.
{kind=link}
{kind=link}
{kind=link}
In the beginning, it was not possible to use the TrueBeam integrated gating cameras and Catalyst at the same time, due to camera interferences. For instance, it was not possible to position a breast patient with a Deep Inspiration Breath Hold (DIBH) plan. The reason was that the frequency bands of the TrueBeam gating cameras and the Catalyst cameras partly overlap. C-Rad successfully installed filters on its scanners to solve the problem.
Notes
1We describe the Varian integration status as of December 2014. Catalyst software version is 5.0.1, and Catalyst does not communicate with TrueBeam at all. In particular, our Catalyst currently does not send any "beam hold-off" commands to TrueBeam, when cMotion detects excess movements during treatment. An integration via TrueBeam's ExIO interface (External IO) is work in progress. It will probably require TrueBeam version 2.5.
2The initial isocenter error should be within 5 cm for Catalyst to give correct calculation results.
3This also includes couch rotation, pitch and roll.