
The light field (LF) of a medical linear accelerator is used to display the position of the radiation field (RF) on the patient skin. Although it is gradually losing it's importance due to IGRT, checking the LF/RF congruence is still mandatory in current QA protocols1.
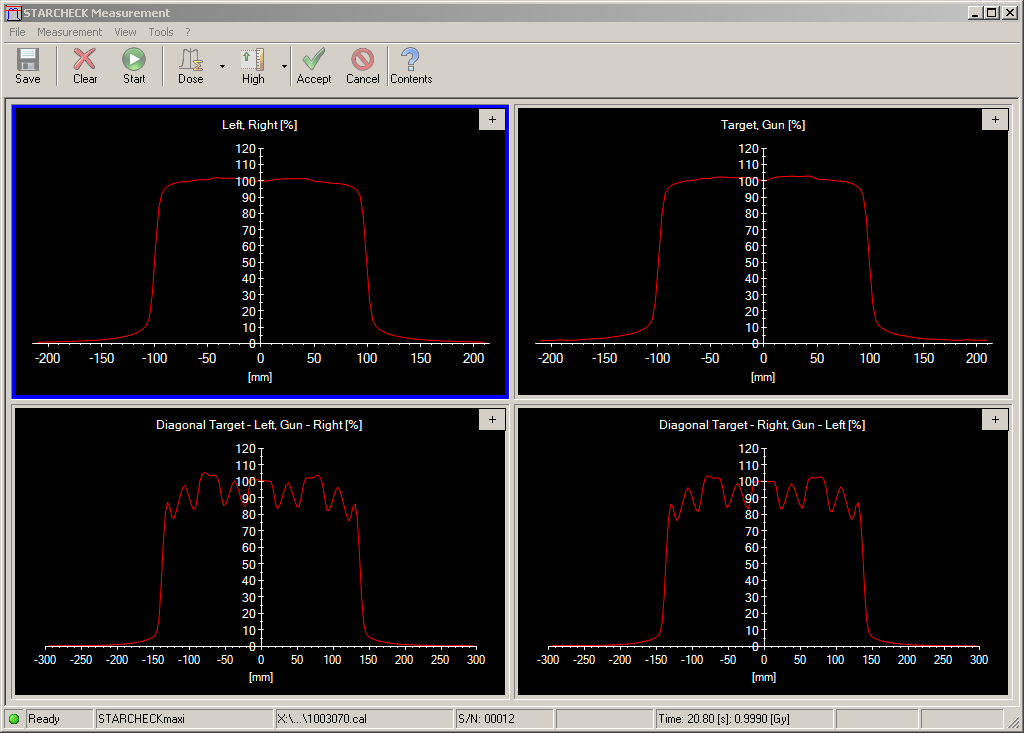
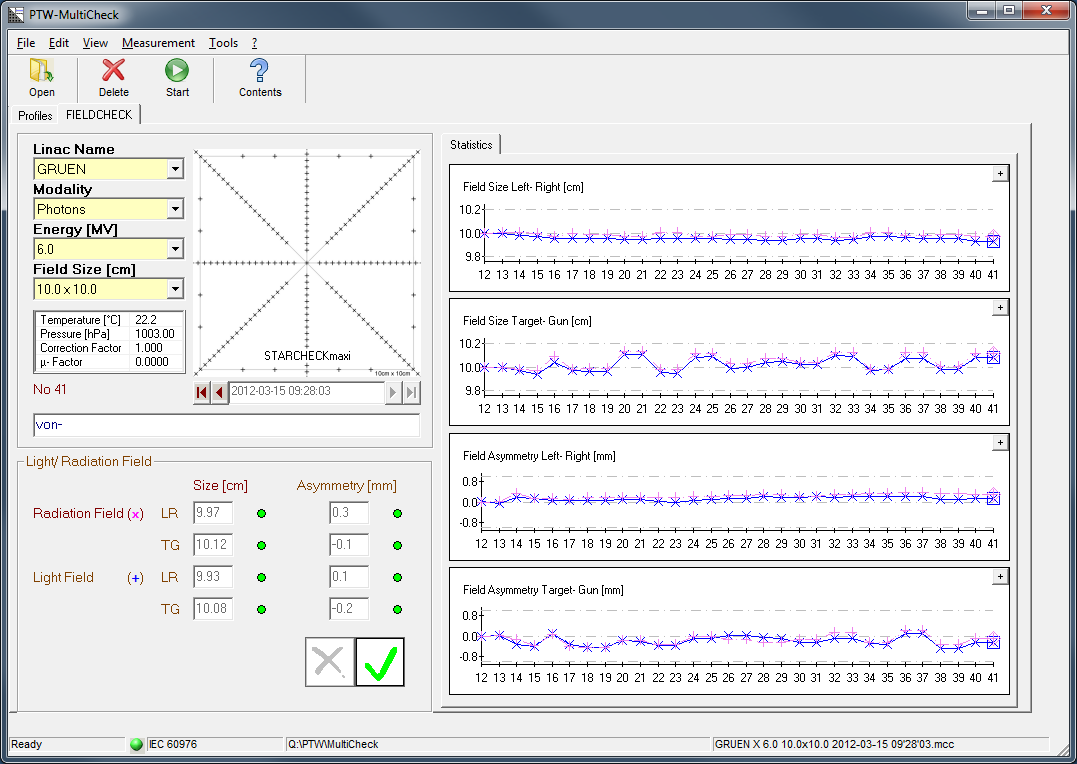
After following the standard procedures (see sidebar) for many years, we entered the post-imaging era in Feb 2011 with a new dosimetric approach that works without images. It uses the FIELDCHECK test object, the STARCHECKmaxi and MultiCheck software Version 3.4, all from PTW. Here is a typical MultiCheck screenshot:
The Principle
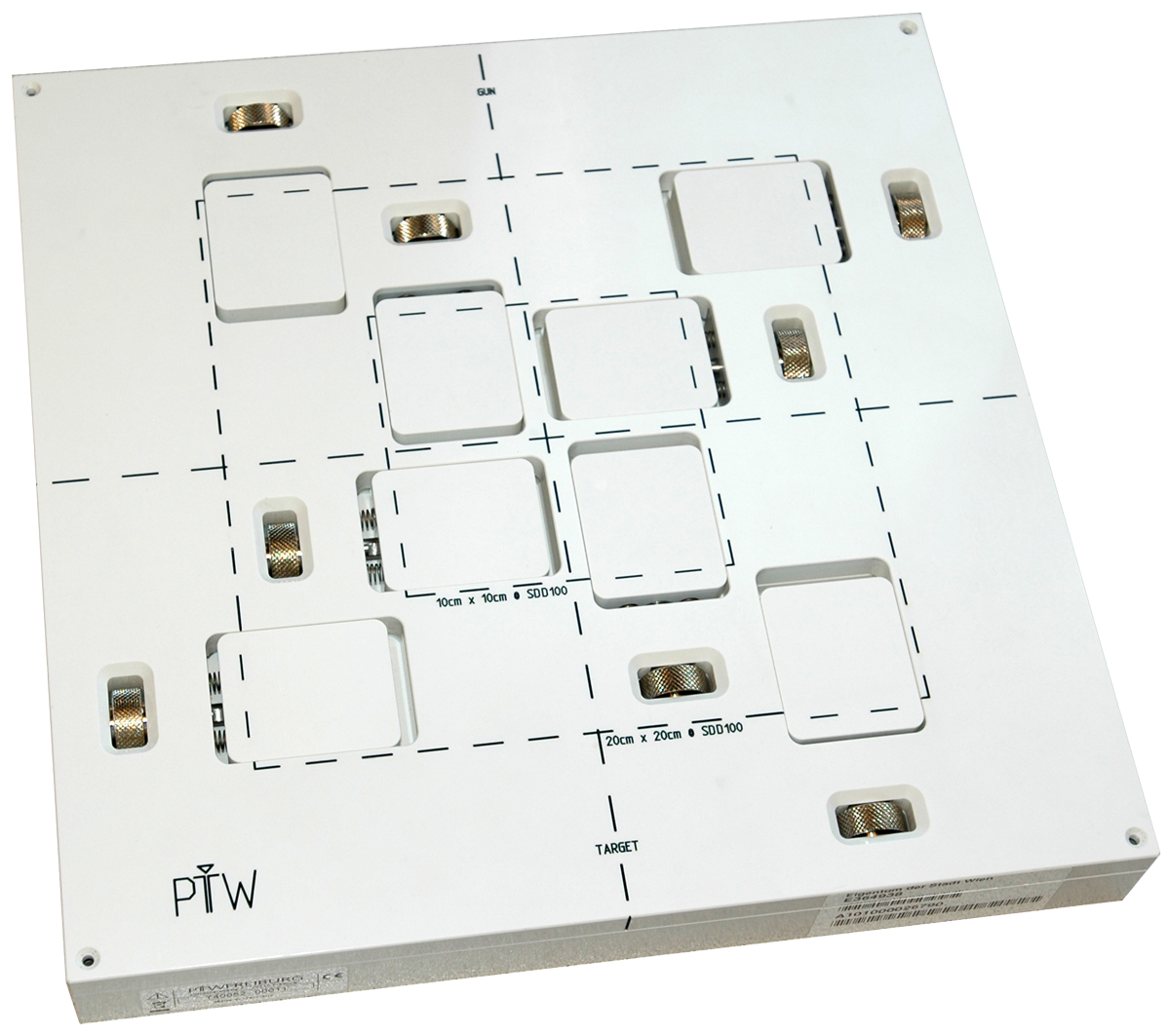
First the STARCHECKmaxi is set up on the treatment table and precisely aligned with the lasers and LF cross-hairs. Then the FIELDCHECK is placed on top of the maxi.2 After the linac has moved the jaws to the target field size (10 x 10 cm or 20 x 20 cm), four movable blocks of the FIELDCHECK have to be adjusted by the user to match the LF edge.
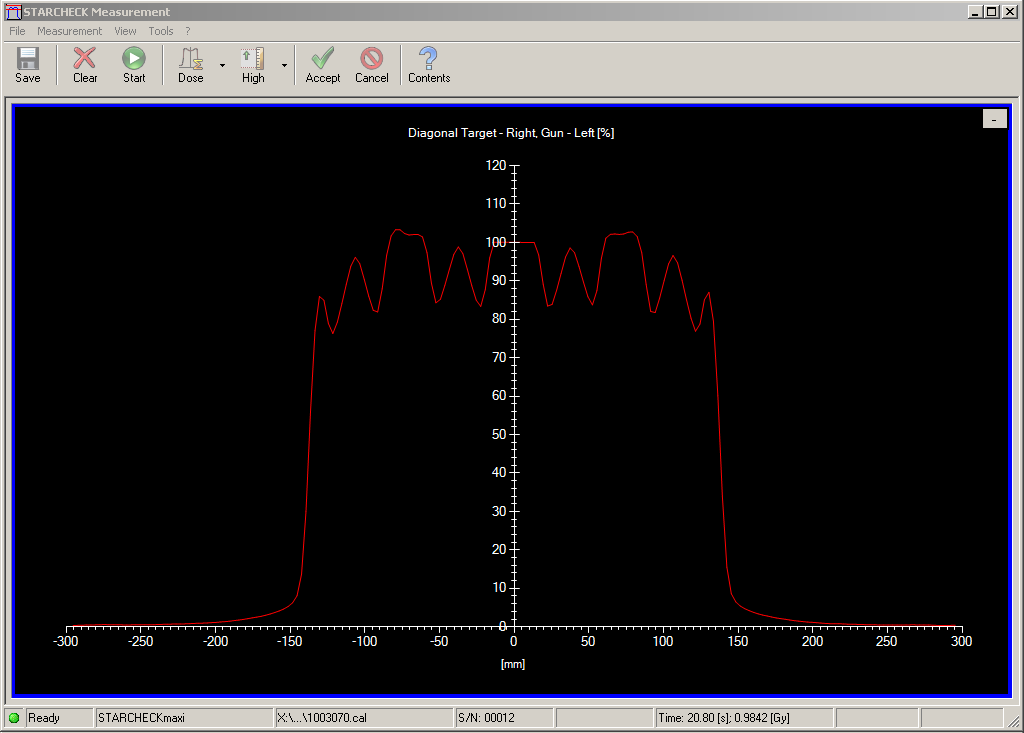
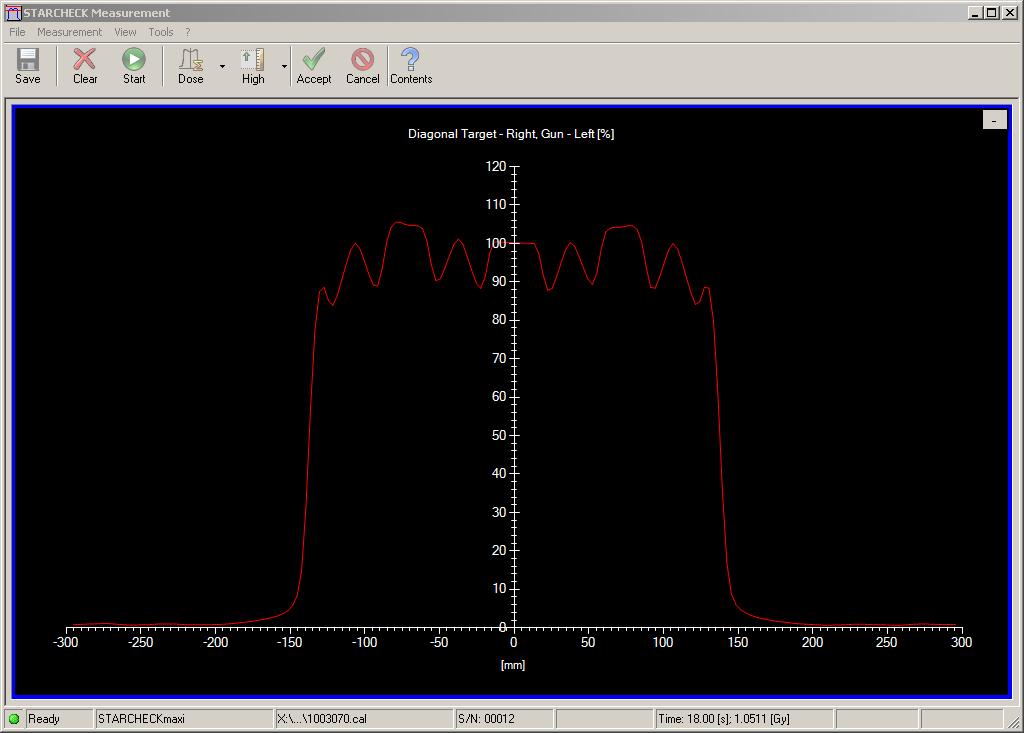
When the field is measured (we use 100 MU @ 600 MU/min), the maxi acquires four profiles simultaneously, which are automatically evaluated by MultiCheck software: The inplane and crossplane profiles (which are acquired under homogeneous parts of the FIELDCHECK) are used to determine the radiation field size. The diagonal profiles on the other hand are "distorted" by metal wedges which are part of the FIELDCHECK's movable blocks. By analyzing these profiles, the software can calculate the LF size with high precision, see the poster by T.Perik et al.
Results
Starting in March 2011, we acquired data sets on two machines (Clinac 2300C/D, S/N 156 & 157) for two energies (6 MV, 15 MV), two field sizes (10 x 10 cm, 20 x 20 cm), and two source-detector distances (SDD = 100 cm and 150 cm3). For each field size, we made two successive shots, to check reproducibility.
Example 1: 6 MV, 10 x 10 cm, SDD 100 cm
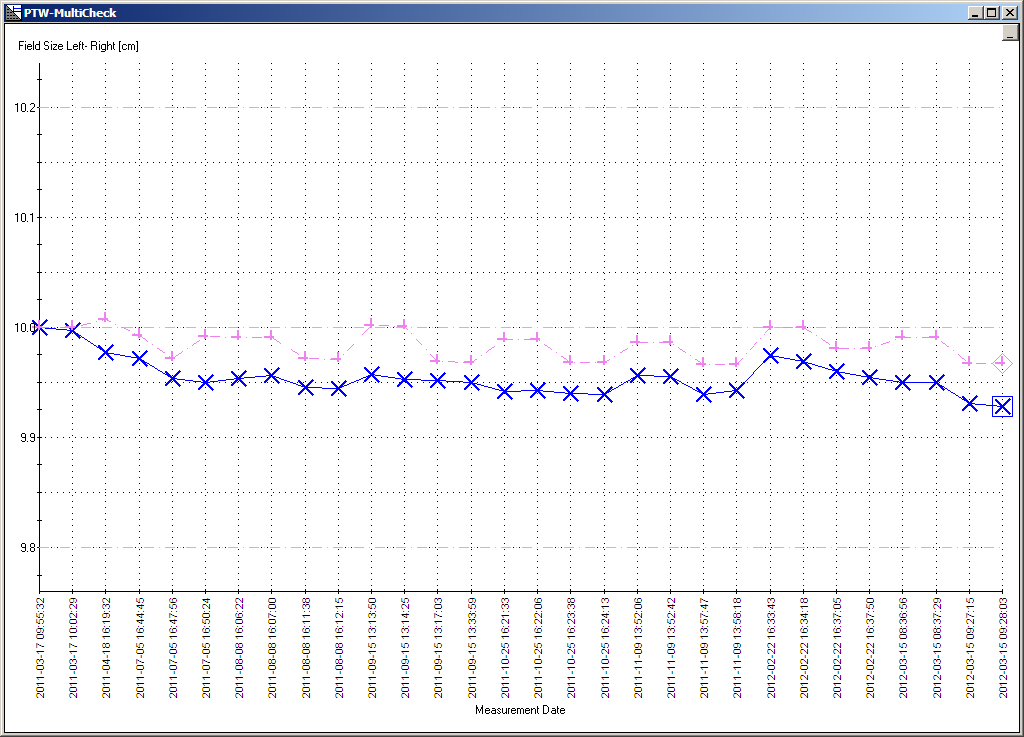
Whereas all deviations regarding crossplane field size, inplane asymmetry and crossplane asymmetry were below 1 mm, the inplane field size showed some hysteresis. Depending on the direction of jaw movement to target field size, measured field sizes were either smaller (if the Y jaws closed in from larger fields) or larger (if Y jaws opened from smaller fields). In direction of movement, they "overshot" a little:
{kind=link}
{kind=link}
{kind=link}
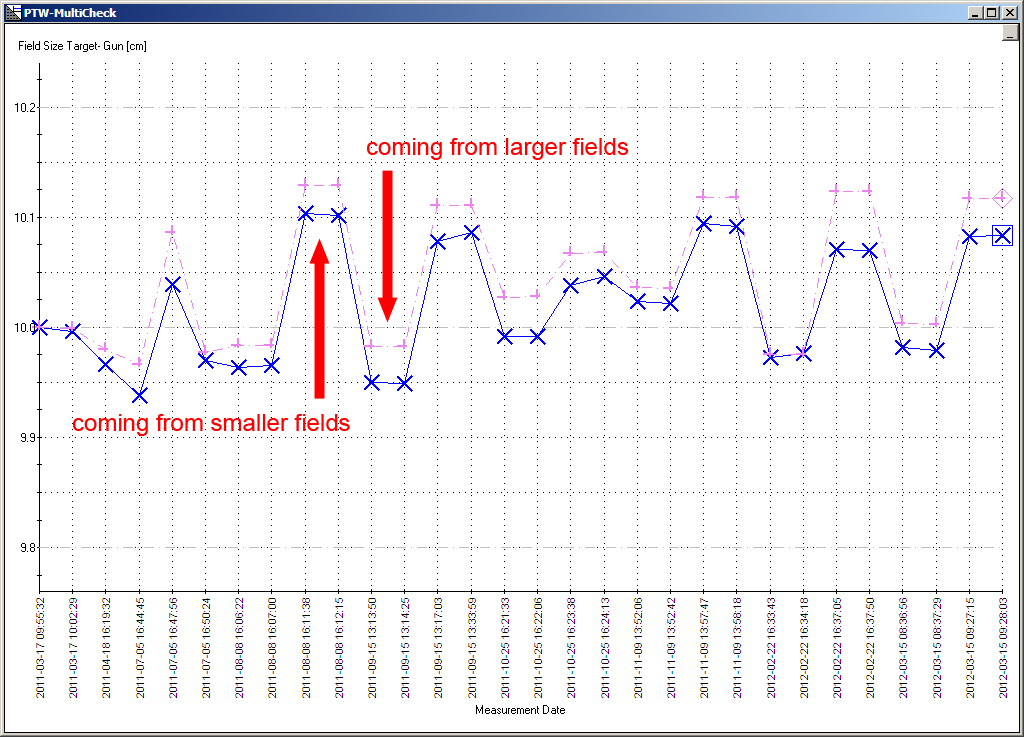
The amplitude of this hysteresis was in the order of 1.5 mm (see graph).
Each target field size was measured twice, and with either direction of jaw movement. This way a possible change in the Y-jaw hysteresis (e.g., due to increasing play in the readout potentiometer) could be safely detected.
The reason why hysteresis was not observed in the crossplane direction (X jaws) is probably due to the smaller distance of the Y jaws from focus: a small play in the readout potentiometer has a larger impact at isocenter distance for the Y jaws than for the X jaws.
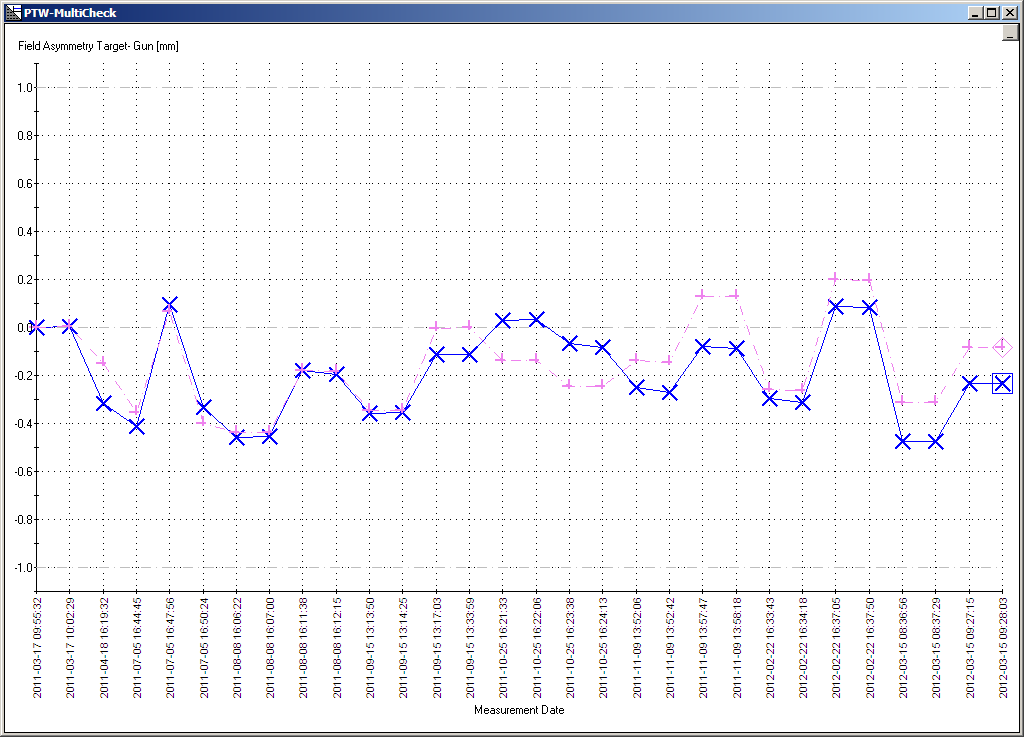
By taking a closer look at field asymmetry, it became immediately clear that mainly the Y2 jaw of this specific linac showed the hysteresis. The reaction of Varian was that the hysteresis amplitude is within specs.
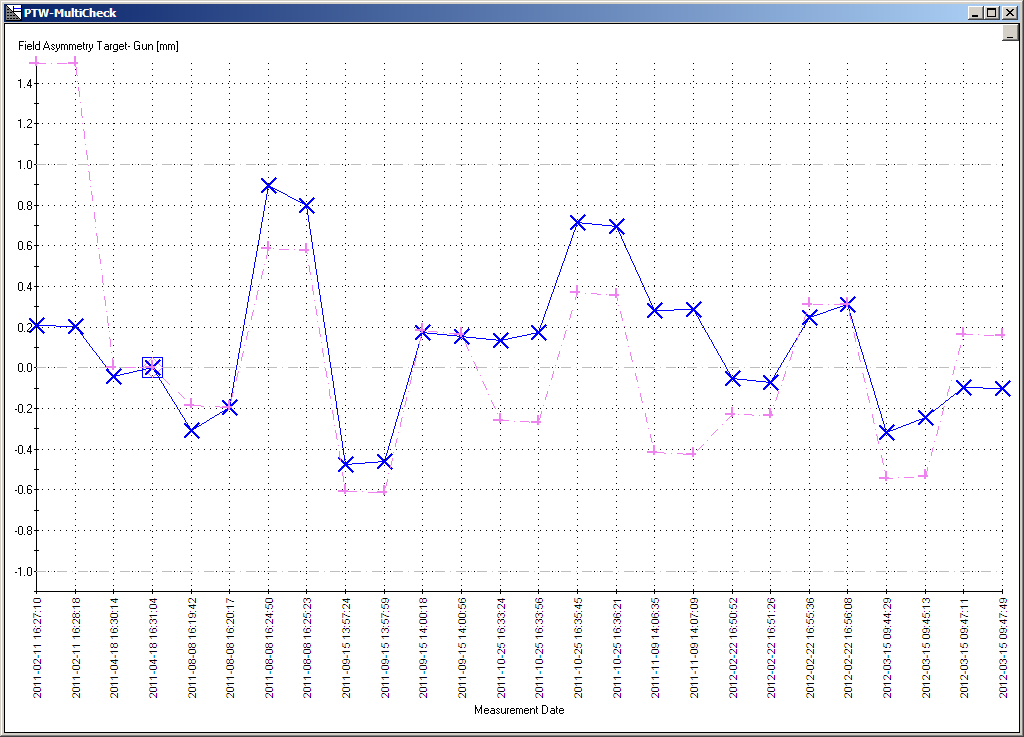
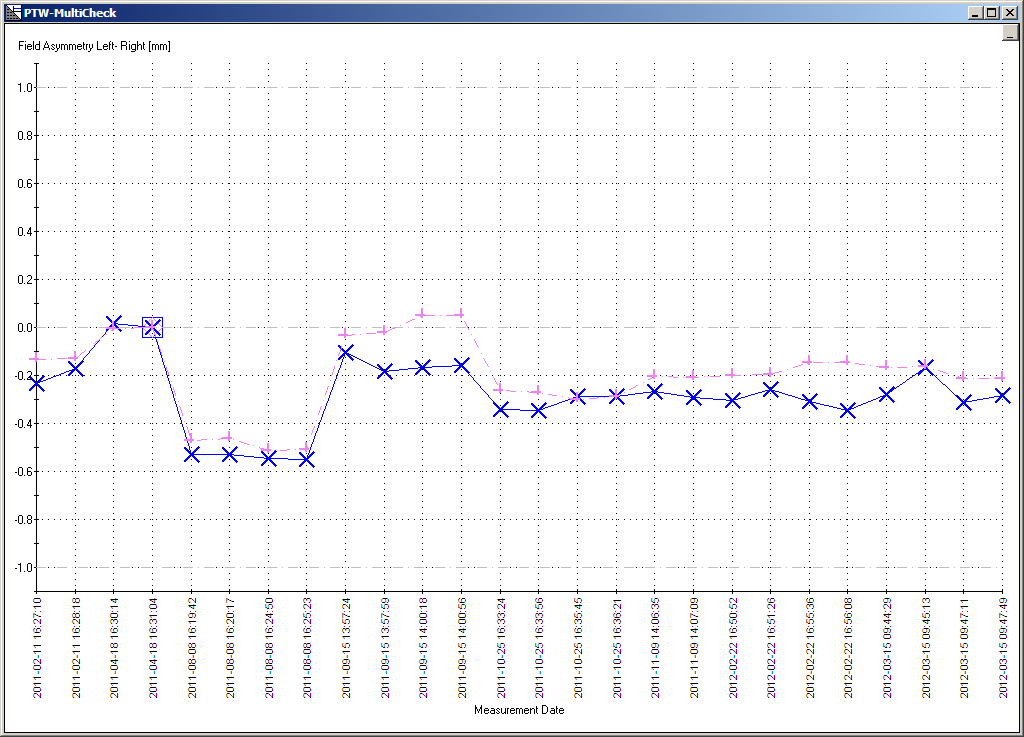
Example 2: 15 MV, 20 x 20 cm, SDD 150 cm
Although FIELDCHECK is not designed for SDDs other than 100 cm, it was no problem to measure at 150 cm. For setup, we recorded the CouchVrt reading at SDD 100 cm (e.g. 2.0 cm), added 50.0 cm, and moved the Couch down remotely to the new position, 52.0 cm4. Then we entered the treatment room and realigned the devices with LF cross-hairs. We were not interested in measuring lateral displacements due to non-vertical couch movement, but only the agreement between LF and RF.
In order to measure a 20 x 20 cm field at 150 cm, jaws have to be set to 13.3 x 13.3 cm at Isocenter. However, we defined this field size in MultiCheck as 20 x 20 cm.
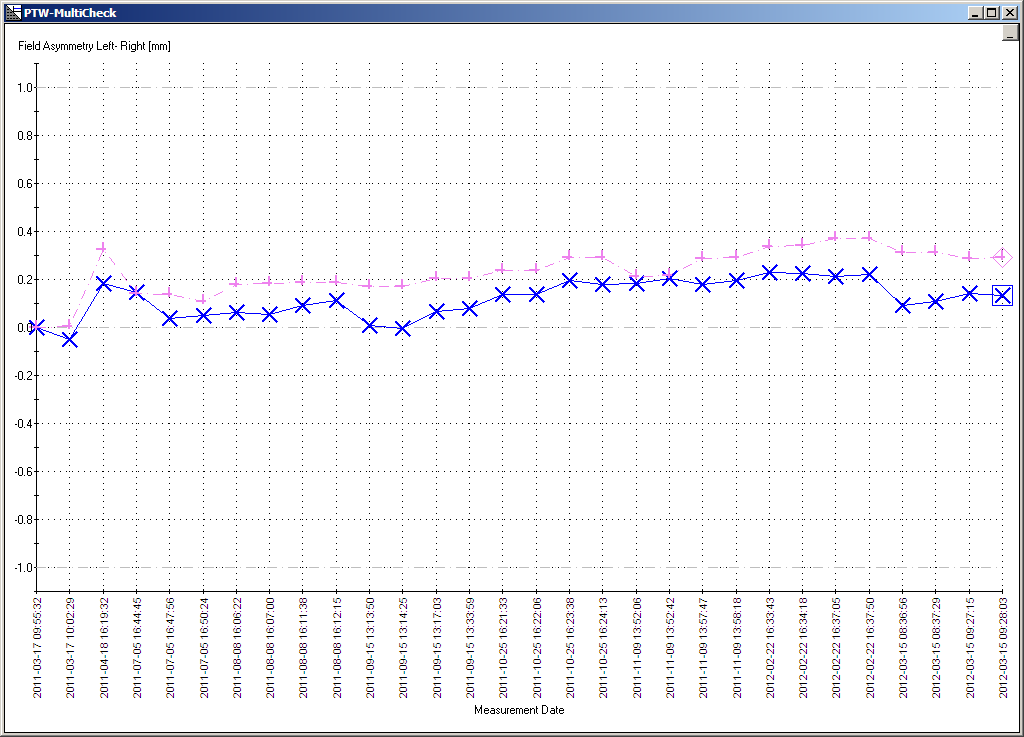
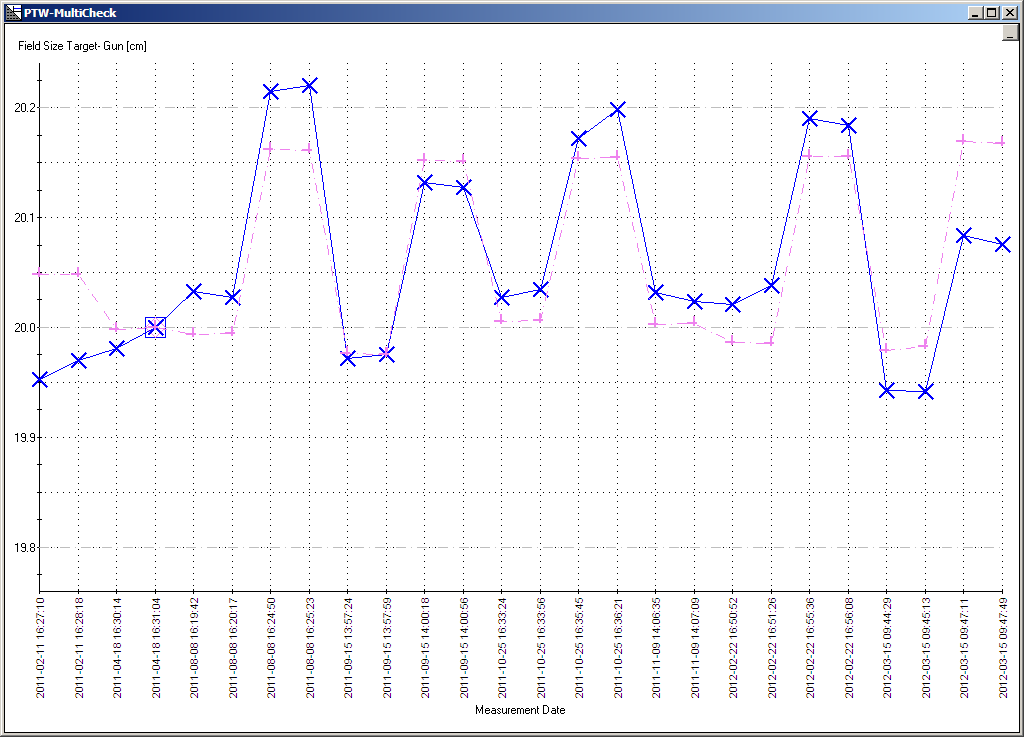
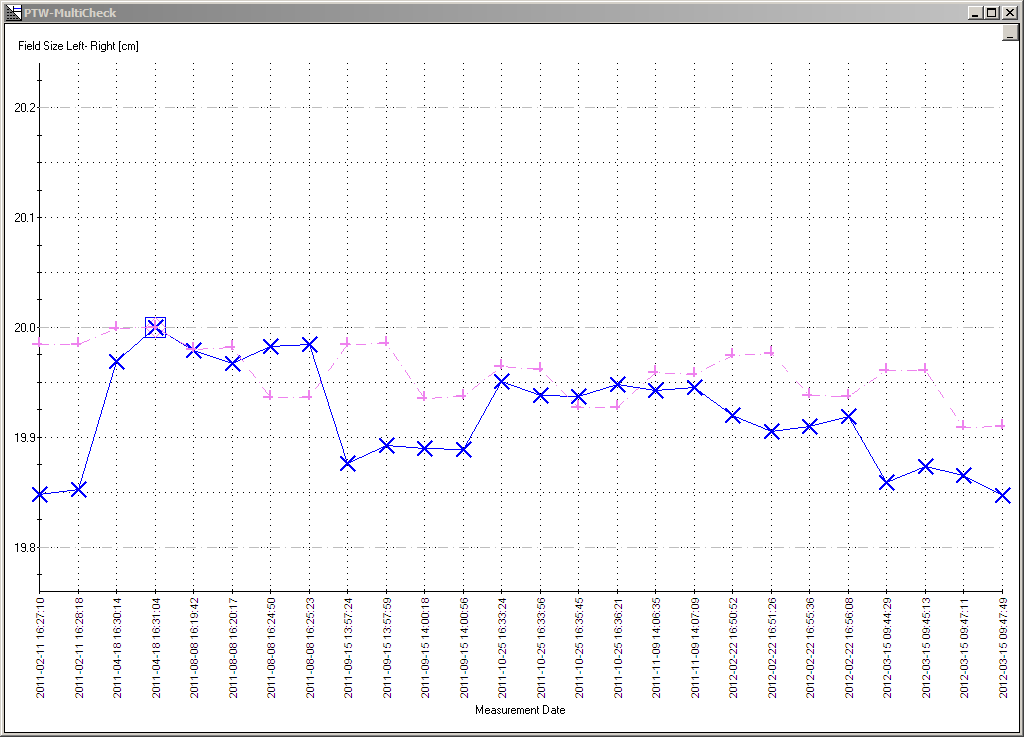
Here are the results for inplane field size, crossplane field size, inplane asymmetry and crossplane asymmetry. The square indicates the reference measurement.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
After the devices have been properly set up, LF/RF measurements are quick, easy, accurate and reproducible. The only user-dependent factor is the judgement of the LF edge, when the user moves the four blocks of the FIELDCHECK. It requires some routine to get reproducible results at the 0.1 mm level. If different users work on the same dataset, larger variations can be expected for the LF.
We hope that some day a device will be available that is capable of "measuring" the LF and the RF at the same time, without being influenced by the "human factor".
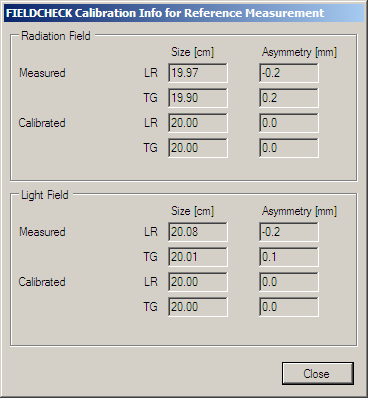
Periodic measurements are always compared against a "reference" regarding field size and field asymmetry, for both the radiation field and the LF. This means that measurements (and the displayed deviations) are never "absolute", but have always to be seen "with respect to the baseline". Therefore, care must be taken when interpreting the results of a later routine check: any asymmetry or field size deviation which exists at the time of the baseline shot will be zero from now on.
However, displaying the reference measurement (here for 6 MV, 10 x 10 cm, Isocenter and 15 MV, 20 x 20 cm, SDD 150 cm) shows absolute values. This can, at least in principle (not within MultiCheck software), be used to get "absolute" values for all later measurements.
{kind=link}
{kind=link}
Two notes regarding the hysteresis effect:
- It is generally a good idea to leave some note in the comment field of each measurement which indicates the direction of jaw movement to target field size, e.g. "from+" or "from-". Otherwise it is difficult to interpret the results later on.
- The direction of jaw movement to target field size during the reference measurement will dominate deviations of later periodic measurements.
A limitation of the described method is that it currently works only for Gantry 0°. To perform such measurements at 90°/270°, a holder would have to be constructed with the ability to rotate the whole assembly (FIELDCHECK, STARCHECKmaxi and the connecting frame) to the upright position - without any mechanical play. This would be quite a challenge for the big and heavy maxi, and would be somewhat easier to accomplish with the smaller STARCHECK.
According to QA protocols, measurements at Gantry 90°/270° have to be performed. For this reason, we still take the 90°/270° shots with the aS500 port imager, as described in the sidebar.
1The Austrian standard S 5290-1:2011-10-15 requires that LF/RF be checked twice a year.
2The adapter frame we use is not necessary if a smaller STARCHECK is used.
3The 150 cm are required by the Austrian QA standard.
4It has to be checked first that the vertical Couch readout is accurate at low couch positions, which are usually not used for patient treatments.