RapidPlan Evolution
RapidPlan was introduced at KFJ more than two years ago. Since then, much time has been devoted to plan optimization and model training.
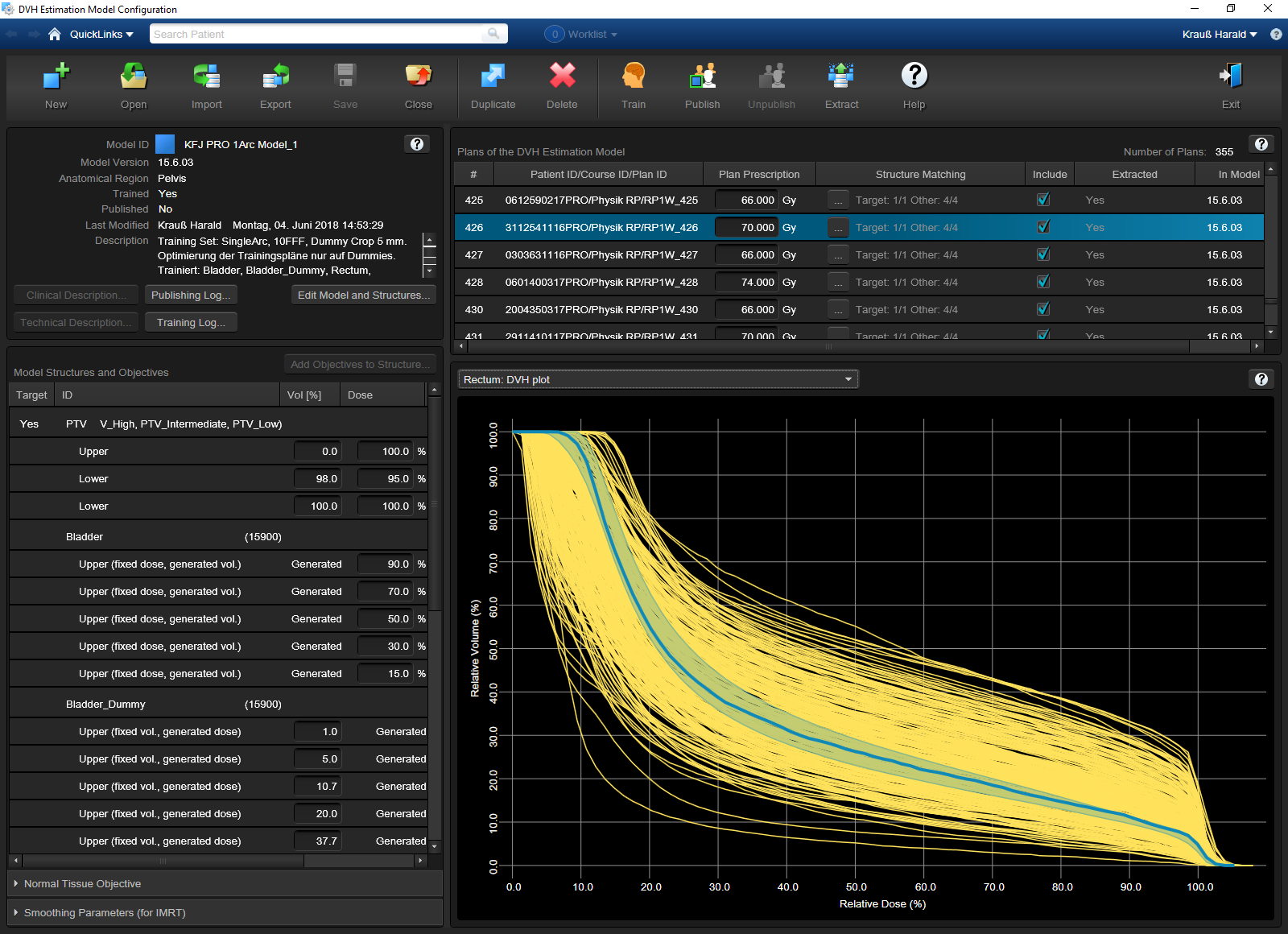
(KFJ single arc prostate model)
At the time of our second report, we were right in the middle of model training, feeding more and more state-of-the-art treatment plans into them. We anticipated that our models got better and better with each new training plan added.
But evolution goes on. Eclipse was updated three times since RapidPlan was commissioned at our institute:
- 13.6 -> 15.0 (Sept 2016)
- 15.0 -> 15.1 (April 2017)
- 15.1 -> 15.6 (May 2018)
Each new ARIA/Eclipse version also included a new RapidPlan version. New algorithms replaced older algorithms, new software features were introduced.
What does this mean for existing models?
From PO 13.6 to PO 15.6
The performance of the optimizer used for inverse planning is a key factor for plan quality. For VMAT (and IMRT) optimization in Eclipse, the PhotonOptimizer (PO) is used.
PhotonOptimizer 15.6 offers several new calculation options1, which might blow the physicist's head off during an attempt to explore them all. First the situation in PhotonOptimizer 13.6, which was in use at the time of RapidPlan commissioning:
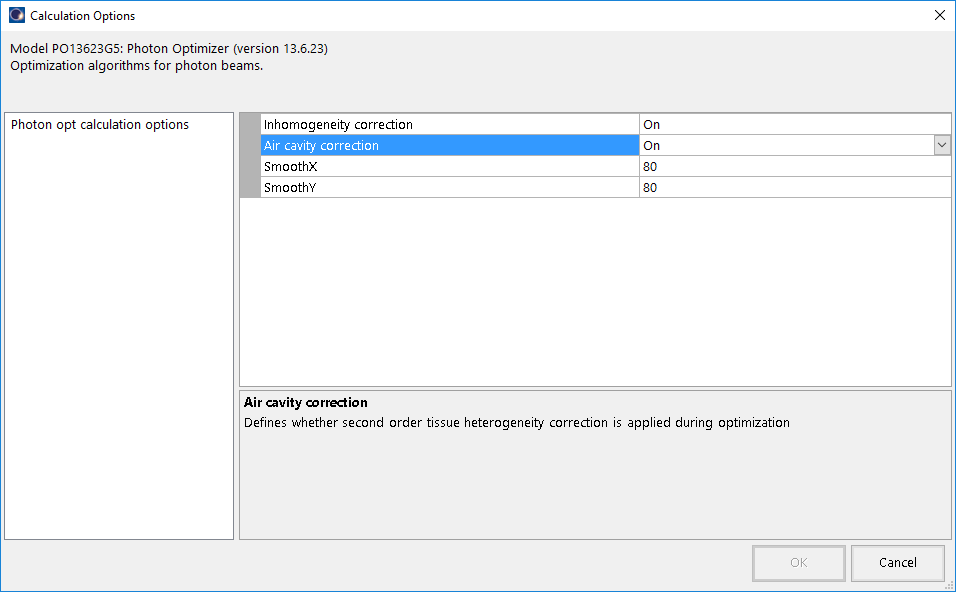
There are only four calculation options. Two of them don't even apply to VMAT2.
Now compare this to the calculation options of the current version:
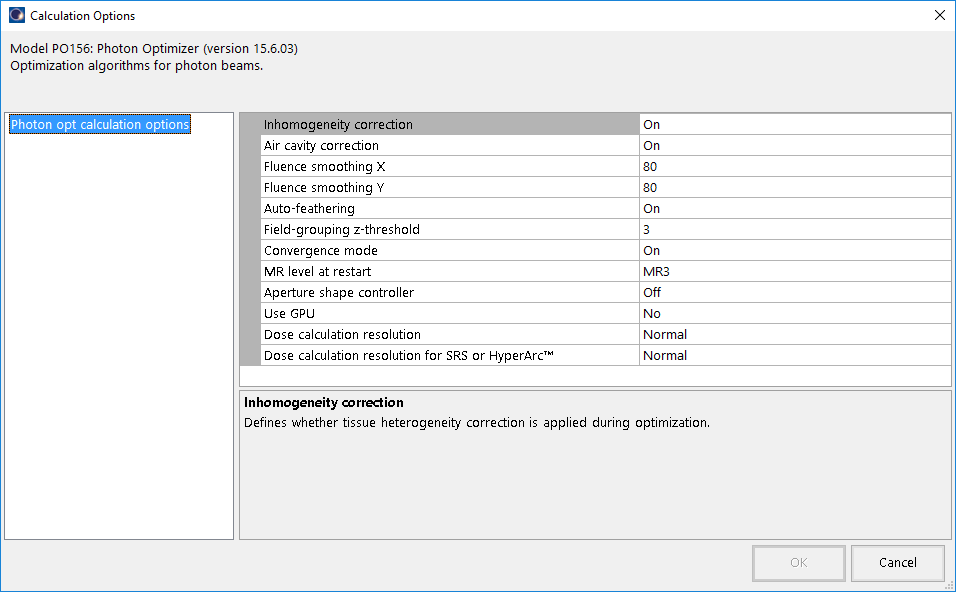
The first four options are the same, but the others are completely new. What does this have to do with existing RapidPlan models, you might ask.
What was once the optimal plan quality, might be only "a good plan" two years later. If there are new calculation options which - if chosen wisely - improve plan quality significantly and these plans are then used to train a model, the outcome (e.g. DVH estimation applied to a new plan) will be different.
Commissioning a new DVH Estimation Algorithm will reveal it: we have seen that the options "Convergence mode" has the biggest impact. It can be set to "Off", "On", or "Extended". "Off" would correspond to the prior to 15.5, where the option didn't even exist.
To explain what convergence mode does, it is best to cite Varian's TPS New Features Workbook 15.5, which can be downloaded from my.varian.com:
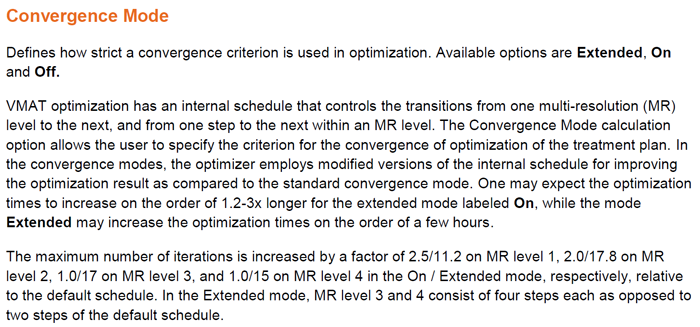
We have experimented a lot with the "On" and "Extended" setting, and we can recommend to set the convergence mode to "On" for daily use ("default settings"). Switching back from MR4 to MR1 manually (which we called "wave" previously) can be omitted. One can walk away during optimization, or do other things. The outcome will still be better than in previous versions. The optimizer simply dwells longer in each MR level, which improves DVH, especially of the targets.
The Problem with Existing Models
While innovation is always good3, a strategy has to be found how to deal with older models. Ideally, all training plans would have to be reoptimized using the latest algorithms, and these plans would then be used to retrain the models.
While this can be an option for smaller models with no more than 50 plans, it is rather unattractive in our case. Our three most frequently used inhouse models currently contain more than 850 plans:
- Prostate model for 10FFF single arc treatments (KFJ PRO 1Arc Model): 355 plans
- Head&neck model (KFJ HNO Model): 226 plans
- Model for palliative treatments of the spine (KFJ 1x8Gy WS Model): 276 plans
Strategy 1: Be Happy!
The simplest strategy is to do nothing and enjoy the fact that the target DVHs are better than they need to be.
What's wrong with that? Well, it can somehow jeopardize the idea of the model.
Example. The idea of our "KFJ PRO ALARA Model" was to spare bladder and rectum as much as possible (used for patients with a special bladder or rectum "history"), giving a clear priority to these OARs. For the PTV however, there was a lower DVH limit which all training plans had to respect: the V95% (the relative structure volume for 95% of prescription dose) should be close to 98%, but not much higher. If it were significantly higher, this would indicate that OARs can be spared even more, or that the plan would rather fit in the general purpose PRO model.
The following image shows such a training plan of the ALARA model. It was optimized with PO 15.0.17 and calculated with AAA 15.0.17. The V95% for the PTV was 98.1%:
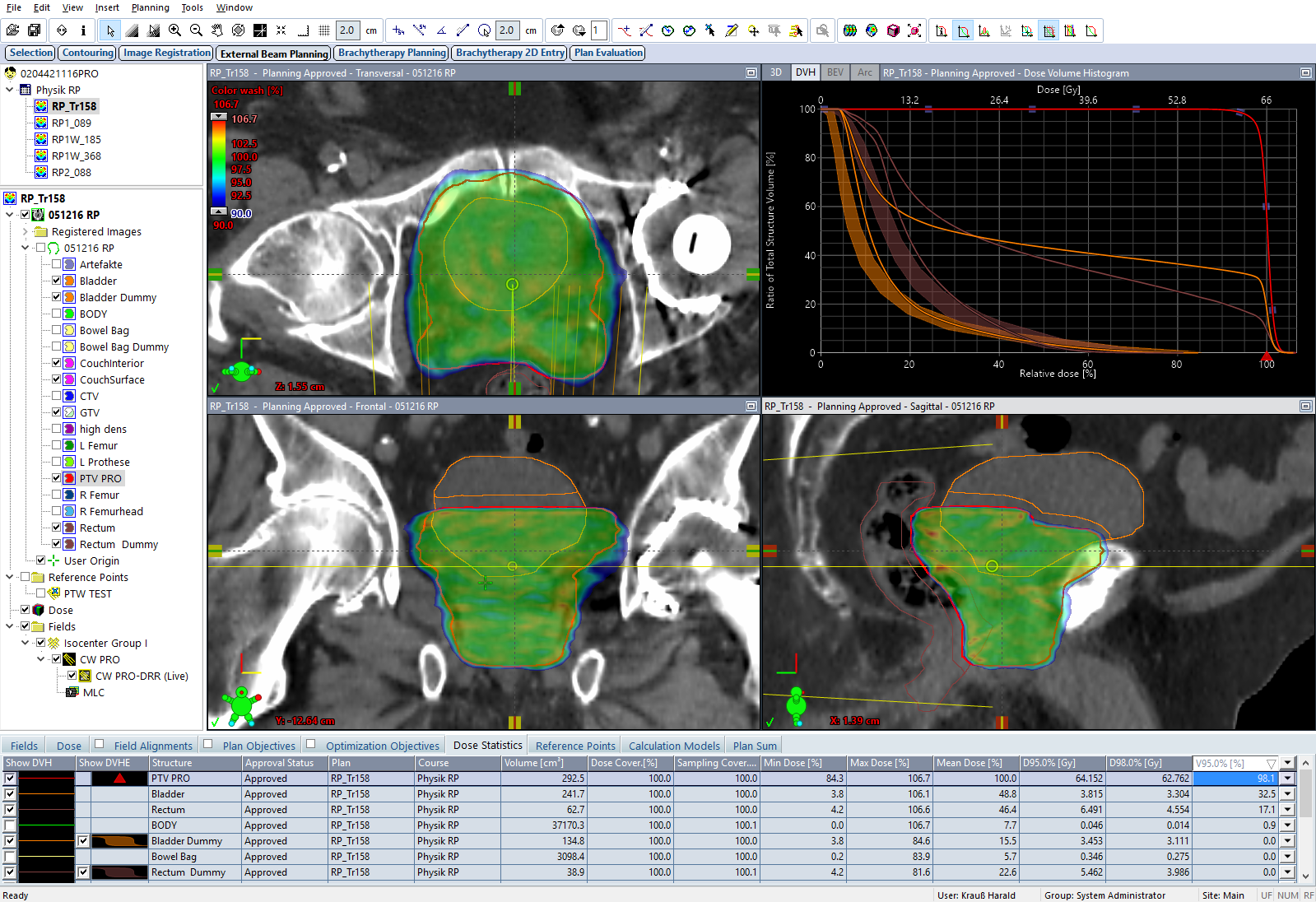
The DVH for the PTV (red line) just touches the required point, which can be seen better in the screenshot of the optimizer:
The ALARA model currently contains 87 training plans, and this one perfectly meets the goals regarding max OAR sparing and min PTV coverage - under the perspective of version 15.0.
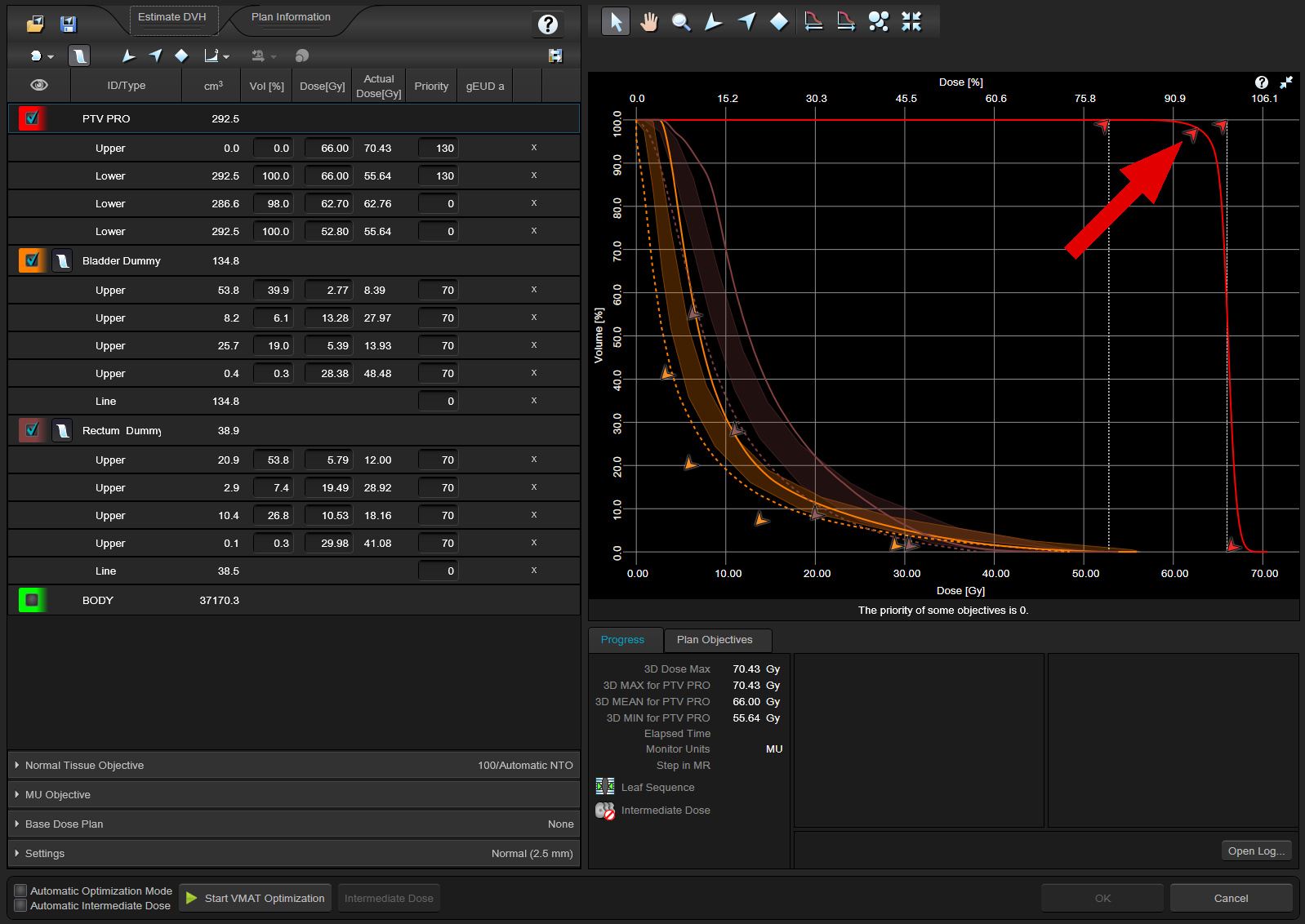
An intermediate step is to take the 15.0 calculated dose and apply the 15.6 ALARA model to get an updated DVH estimation:
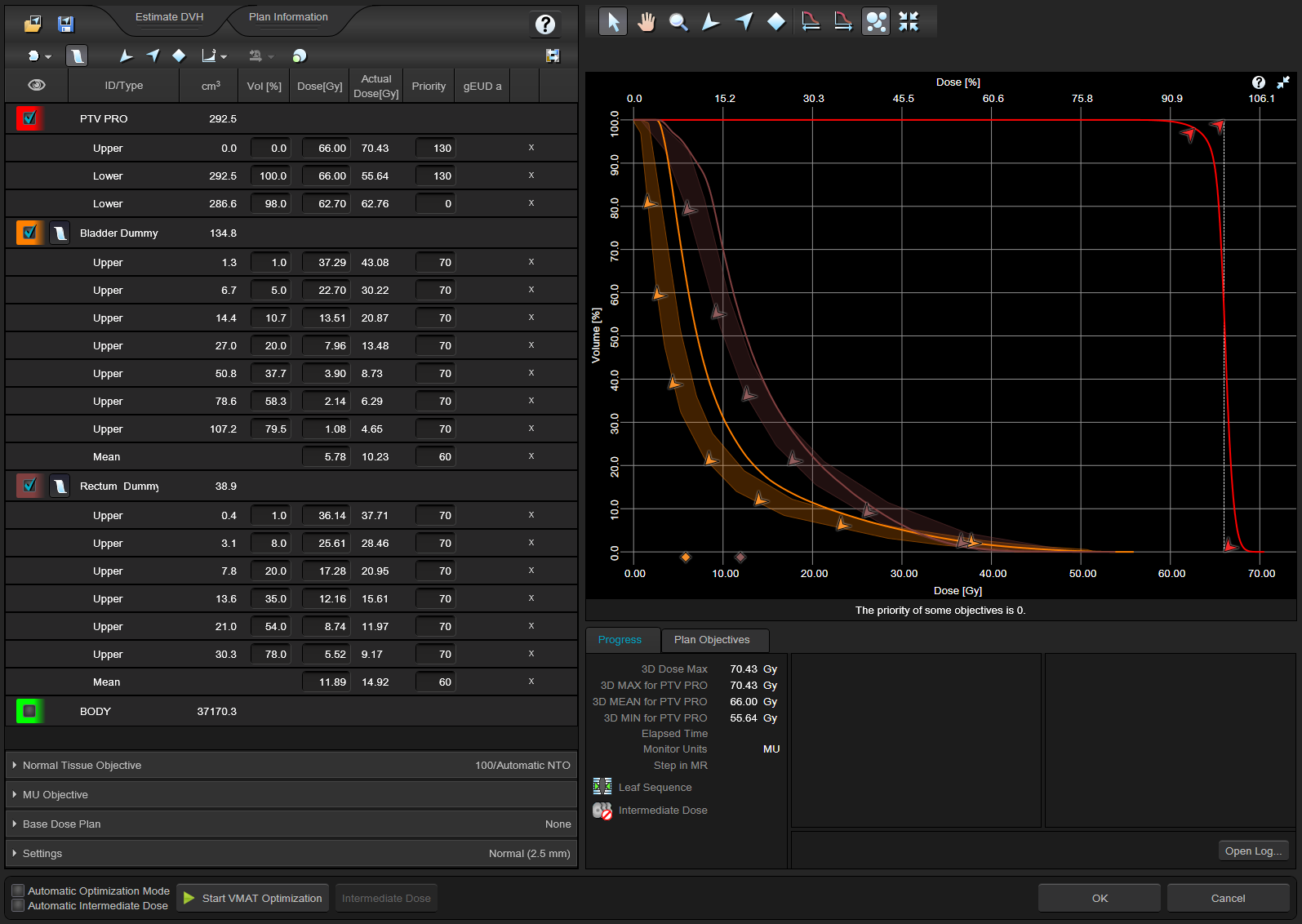
Finally a new optimization is performed with PO 15.6, without touching any objectives. This is similar to the commissioning steps recommended for new DVH estimation algorithms, with the exception that the current plan is already part of the training set. But we are rather interested in the optimization result, which now takes use of the new "convergence mode" option:
At first sight, PTV has improved compared to 15.0. There is now a clear distance between the red arrow at V95% and the PTV curve.
This is confirmed by a DVH comparison of the two plans (squares: plan "Estim156" optimized automatically with PO15.6, triangles: plan RP_Tr158 optimized manually with PO15.0):
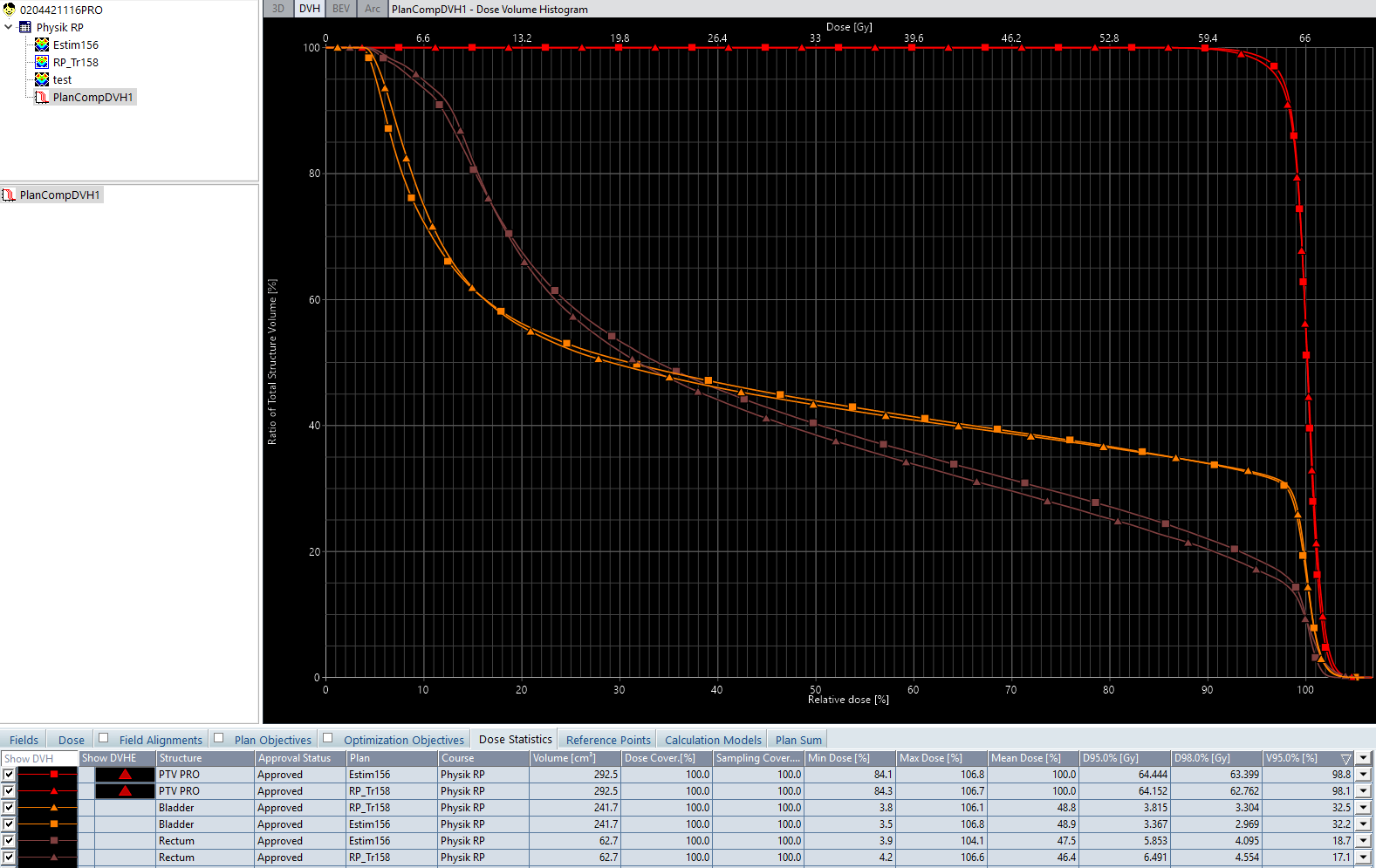
What about bladder and rectum? If one compares mean dose values, bladder is practically the same, rectum with 15.6 is clearly worse. Since PTV15.6 is better than necessary, one might try to tweak the objectives which are generated by DVH Estimation Model (giving higher priority to the rectum). Hovever, after only one test case one must not do that.
Note that this was not a fair comparison of the PO versions, because the 15.0 plan was optimized manually, while the 15.6 plan was not. After manual optimization with PO 15.6, the result is this:
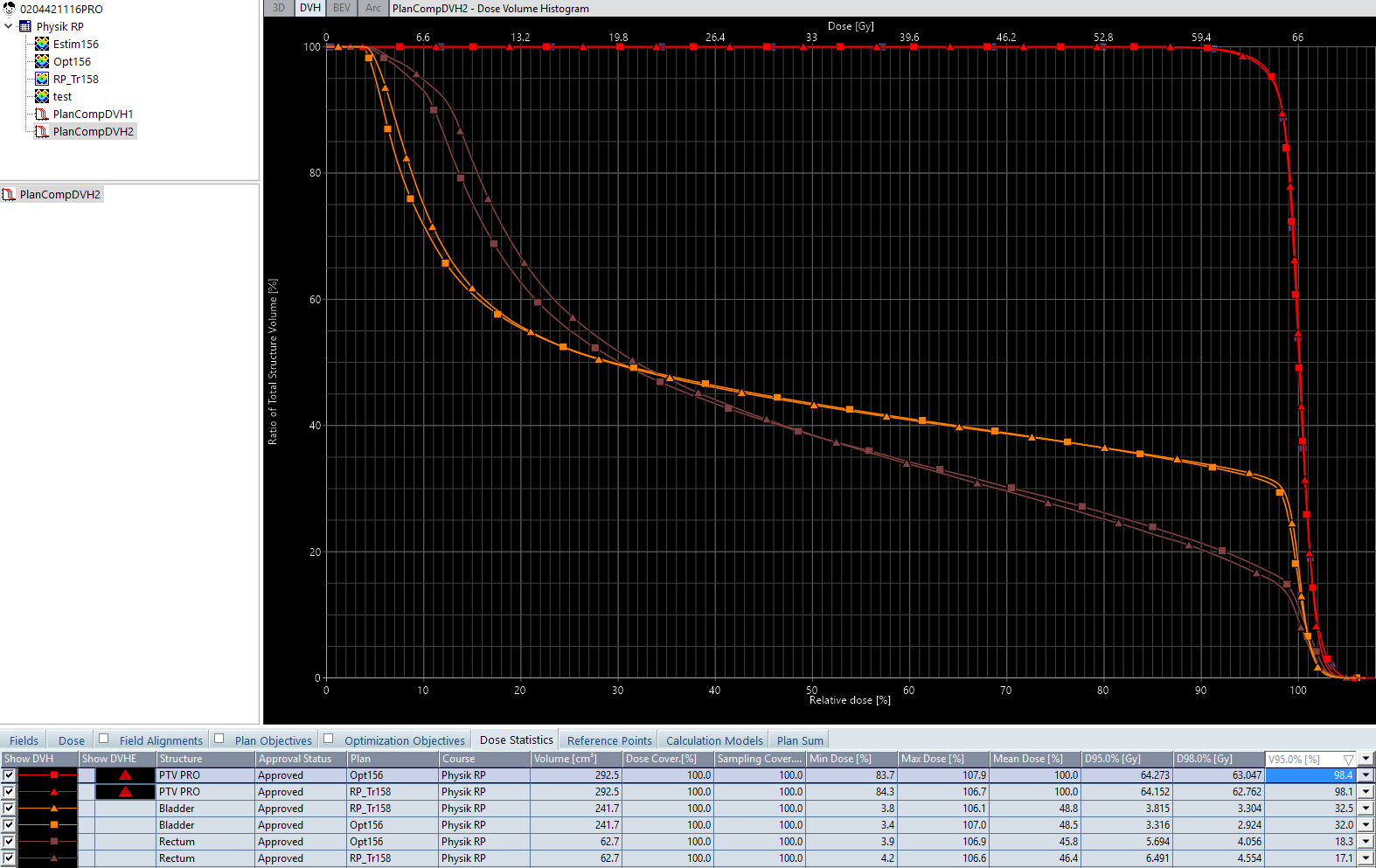
Now 15.6 is better for all three structures, which confirms the general feeling that the performance of the PO 15.6 has improved.
Here is a second example which demonstrates that the PO 15.6 result (squares) is much better than the corresponding 15.0 result (triangles), at comparable PTV coverage:
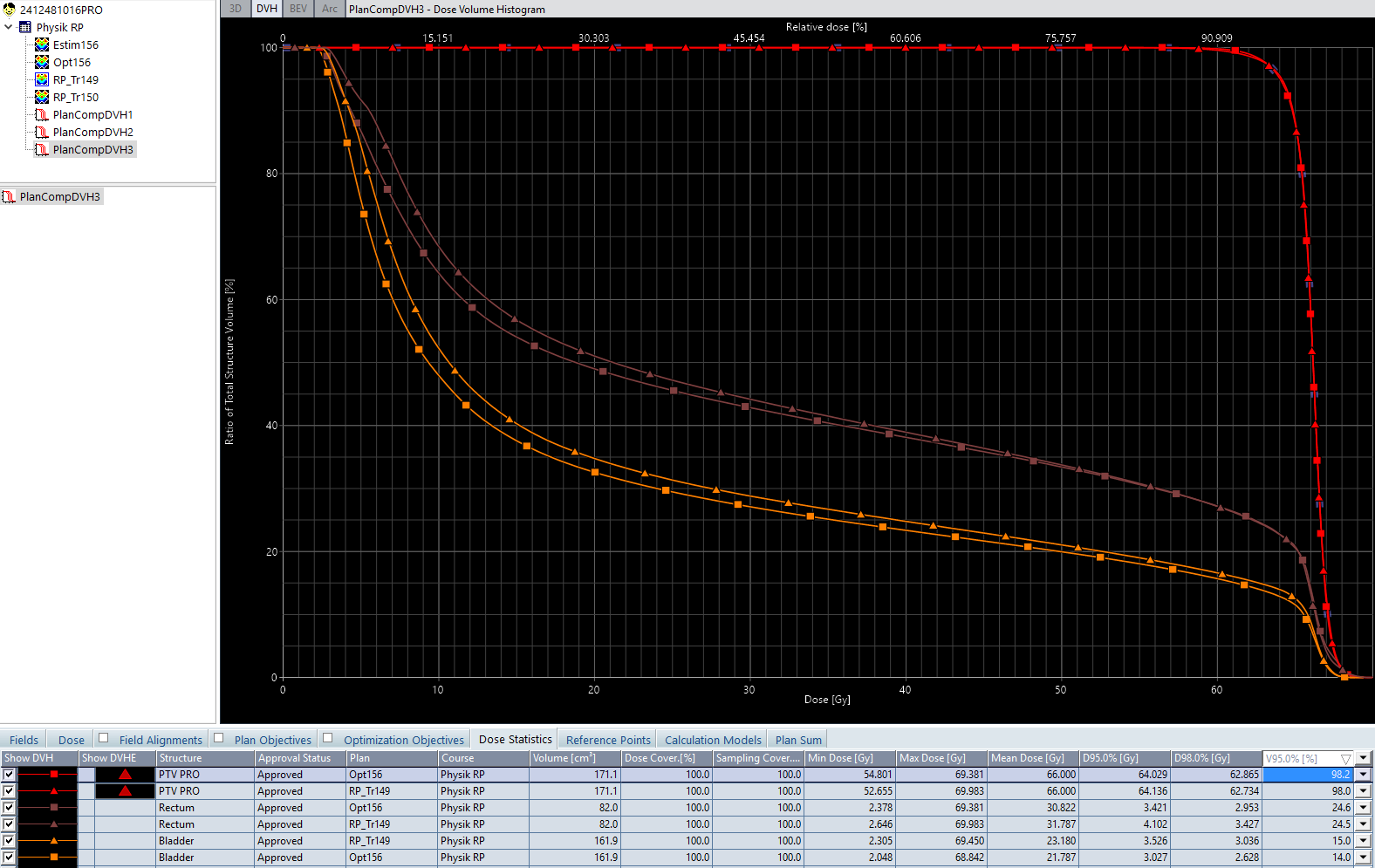
If plans like the last one, manually optimized with PO 15.6, would have been used instead of plans like RP_Tr158 to train the ALARA model, the estimation bands for the rectum would generally be at slightly lower values, simply because PO 15.6 can achieve better results.
Strategy 2: Change Line Objectives to Point Objectives to Gain Flexibility
If a model generates line objectives for the OARs, the position of these lines cannot be changed when the model is applied to a new plan. Replacing line objectives with upper dose objectives is a simple trick to gain more flexibility during everyday optimizations. The estimation error is ignored, but can at least be compensated if needed. We have done that for the ALARA model.
Strategy 3: Add New Plans to Model, Delete Old Plans
This is possible, and it it makes sense if not too many plans are in the model. One could, for instance, add a certain number of plans that were optimized with 15.6, and delete a bunch of old plans (optimized with 13.6). This would refresh the "population" of training plans within the model. But adding 20 new plans to a model which contains 300 old plans will probably not have much impact.
Note that all such reconfigurations also require reverification, revalidation, etc., etc.
Summary
We have chosen two arbitrary plans to demonstrate an evolutionary dilemma: When RapidPlan models are in clinical use, they are sometimes not reflecting the plan quality which can be achieved with up-to-date optimizers because the plans that were used to train the models are "old" plans. Therefore, the models based on these plans are also "old".
Eclipse updates are typically offered once a year. However, not every update contains optimizer innovations. This is why the situation is not as bad as one might guess after reading this article. Plans that were generated with RapidPlan two years ago are by no means "poor" plans. At the time they were created, they were really "optimal".
Notes
1 The options were first introduced in Eclipse 15.5, but we skipped that version. Actually we are talking about 15.5; version 15.6 just added some Halcyon related features.
2 The parameters SmoothX/Y apply to IMRT optimization only.
3 The DVH Estimation Algorithm 15.6 itself contains a lot of improvements too, but here we focus on the training plans.