The Power of Multi-Criteria Optimization
Executive Summary
Trade-Off Exploration, which is based on Multi-Criteria Optimization (MCO), offers the VMAT dose planner a tool to explore a multi-dimensional plan space, or collection of alternative plans. The plan space is generated by optimizing a vector of optimization functions instead of a single objective function. Sliders can be used to continuously explore the resulting Pareto surface1. By doing this, the planner can often achieve a plan quality which is better than that of conventionally optimized plans. Trade-Off Exploration was introduced in Eclipse version 15.5. With version 16.1, it has matured into a valuable tool which can not only increase dosimetric plan quality, but also reduce overall planning time.
Example Prostate Case
The starting point is an existing plan which has been optimized by using the Photon Optimizer (PO). Varian calls this the "balanced" plan. It contains a set of trade-off objectives regarding OAR sparing (bladder, rectum) and PTV coverage. The balanced plan serves as the center of approximation of the Pareto surface.
We usually generate the balanced plan by using a trained DVH estimation model ("RapidPlan") which is applied to the current planning task. However, RapidPlan is not necessary for trade-off exploration.
Our starting plan has the OARs Bladder and Rectum (plus their non-overlapping versions "Bladder Dummy" and "Rectum Dummy"). The PTV should receive 74 Gy mean dose in 37 fractions.
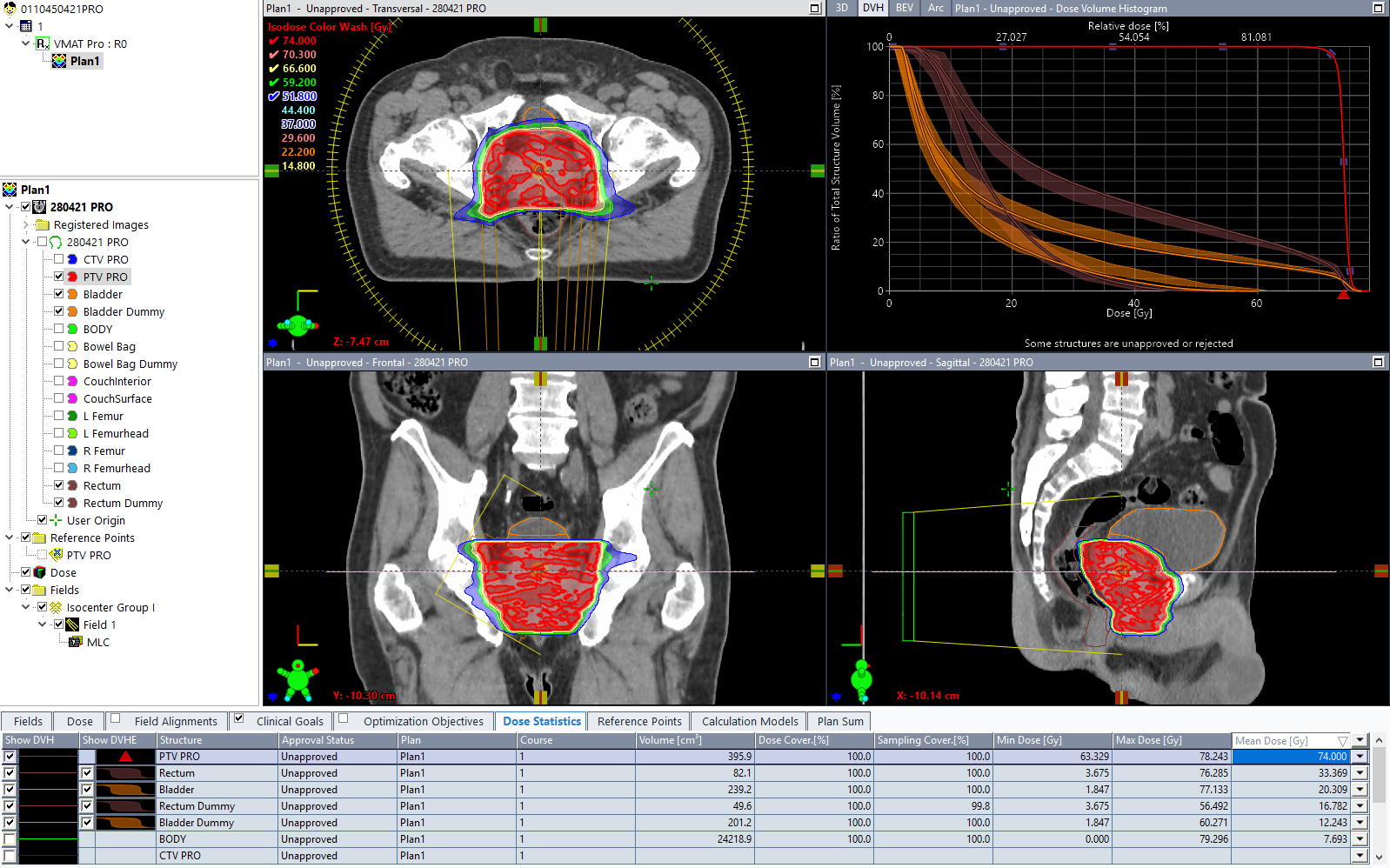
As one can see from the estimation bands in the dose-volume histogram (upper right), this plan was optimized with RapidPlan:
For DVH estimation we used our single arc 10FFF prostate model (upper left):
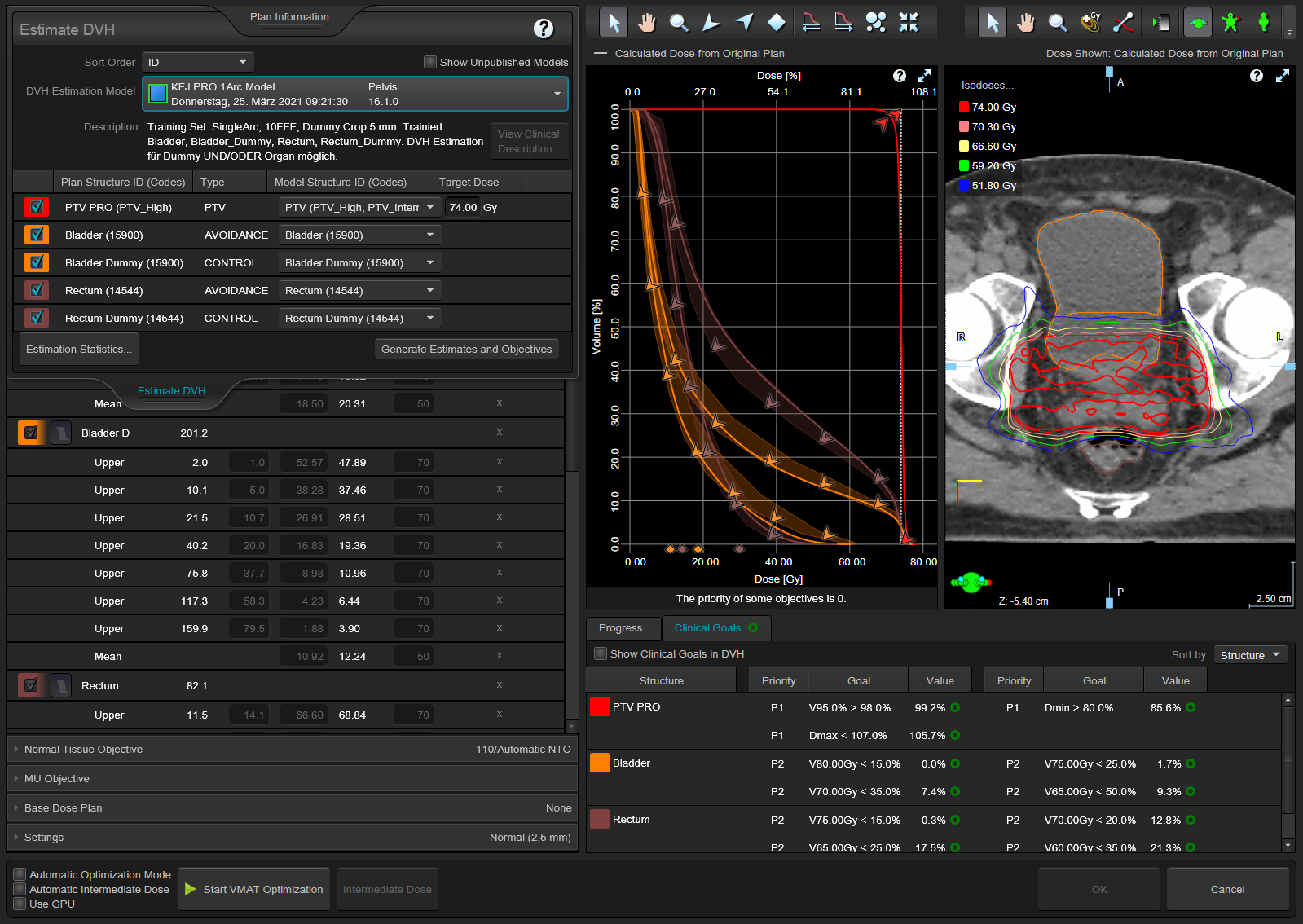
This image also reveals that Clinical Goals are attached to the plan. Clinical goals are very helpful during optimization, because they trigger the permanent calculation of figures which are displayed in the lower right part of the screen.
Not shown here is the small problem of Plan1: it has a 3D Dose MAX of 107.2%, which is higher than the 3D MAX of PTV PRO (105.7%). In other words, there is a small hotspot outside the PTV. Since we want to compare the MCO based plan with the best solution we found manually, we therefore brush up the manual plan, with the strategy we described recently.
The resulting Plan2 (3D Dose MAX = 3D MAX of PTV PRO = 105.8%) is a good plan which we would accept for treatment. But now we want to try trade-off exploration.
In order to save the plan for later comparison, we first copy it to Plan3. Otherwise, trade-off exploration would overwrite the contents of Plan2.
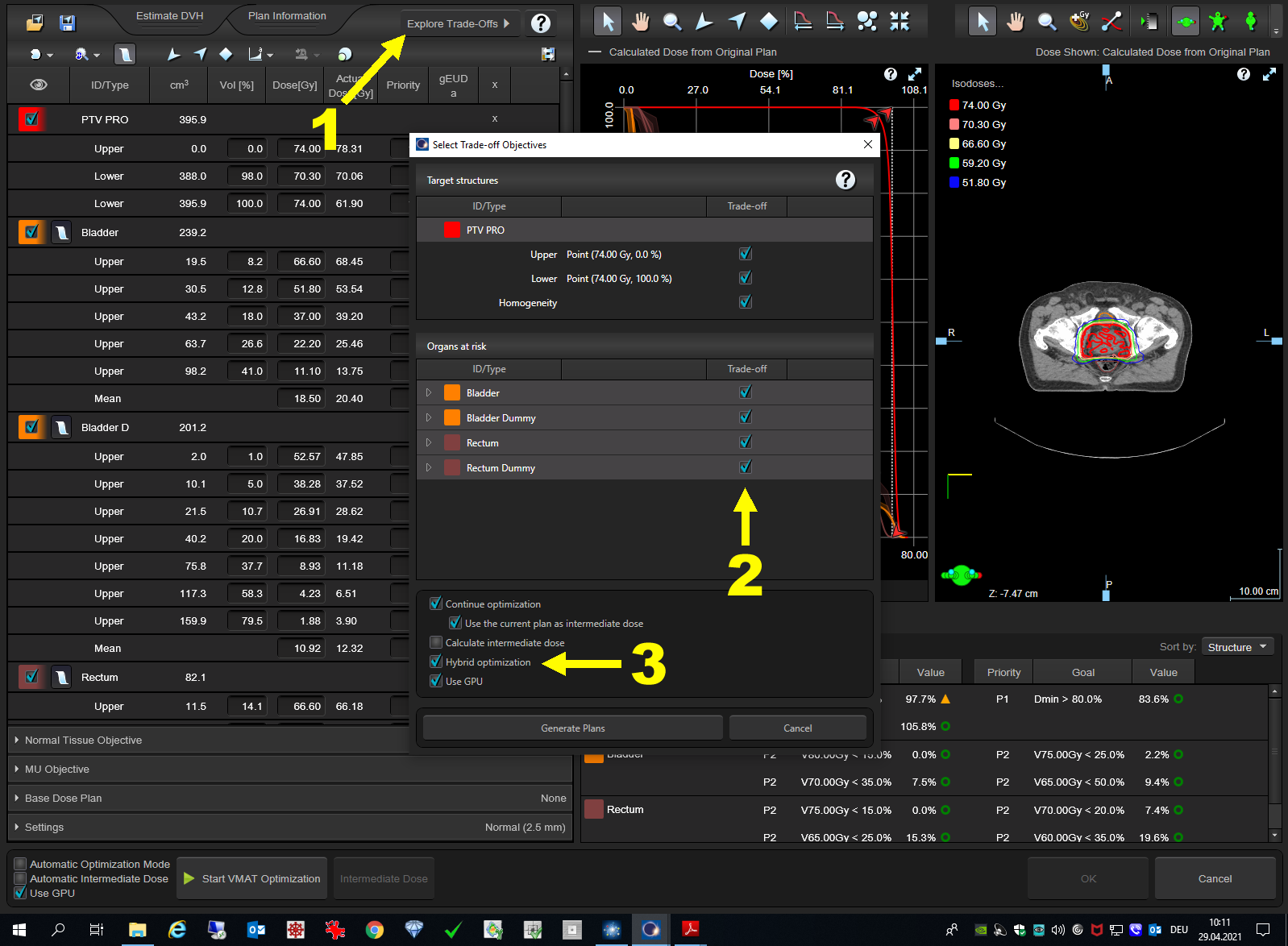
Trade-off exploration is invoked by opening the optimizer (F7), and selecting the "Explore Trade-Off Button" (1). We usually select all checkboxes (2) to get as many sliders as possible. Selecting Hybrid optimization (3) is strongly recommended, otherwise the generation of the plan collection would take hours, especially if no GPU is available.
Then the waiting begins ...
On our system, it takes 2 minutes and 47 seconds until the plan collection is created. This is very reasonable, thanks to the GPU.
The screen which appears next contains one slider for every structure we chose earlier.
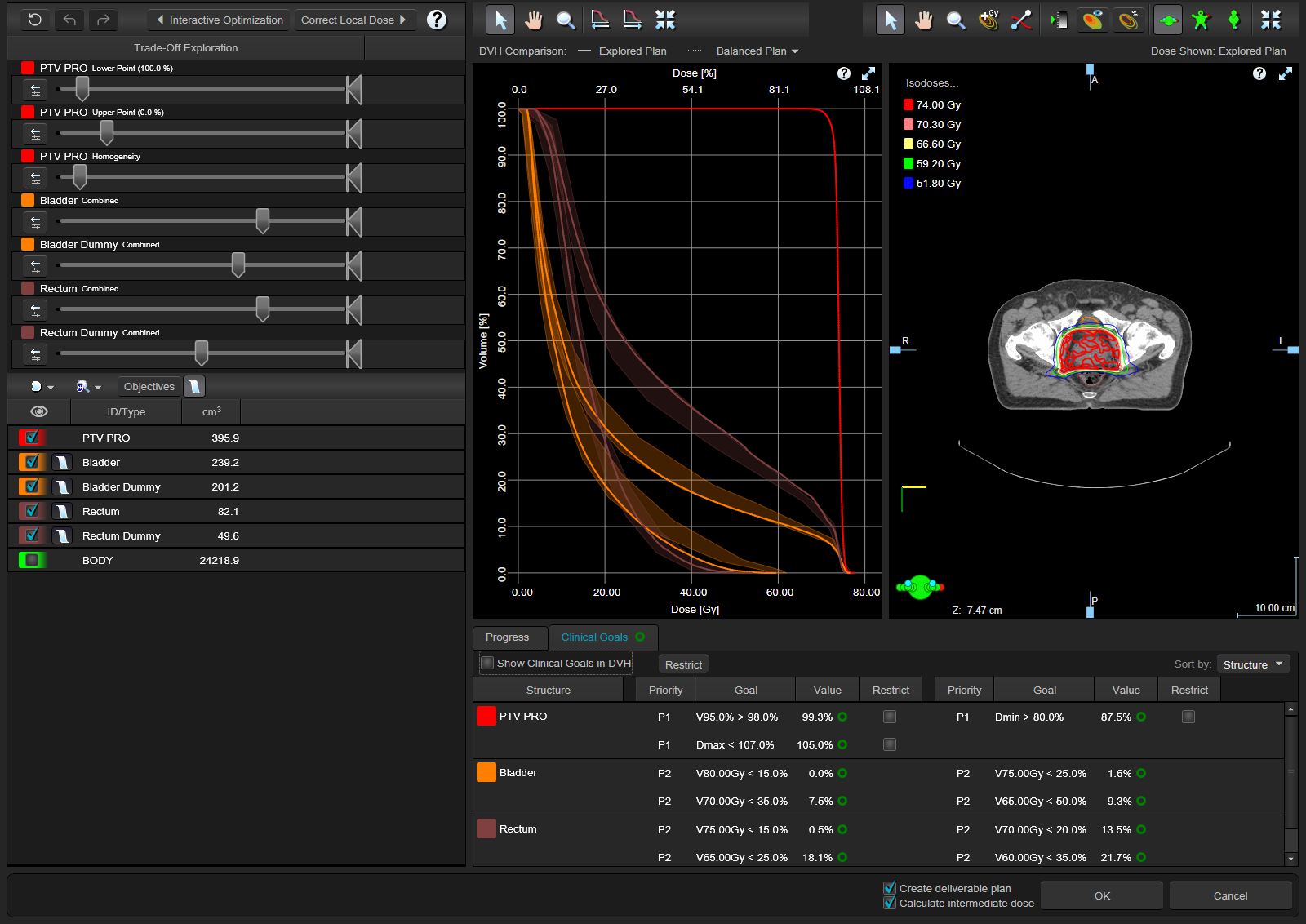
If a slider is moved interactively, all DVH curves update in real time, together with the clinical goal values. This is because the plan collection, or plan space, already exists in the background.
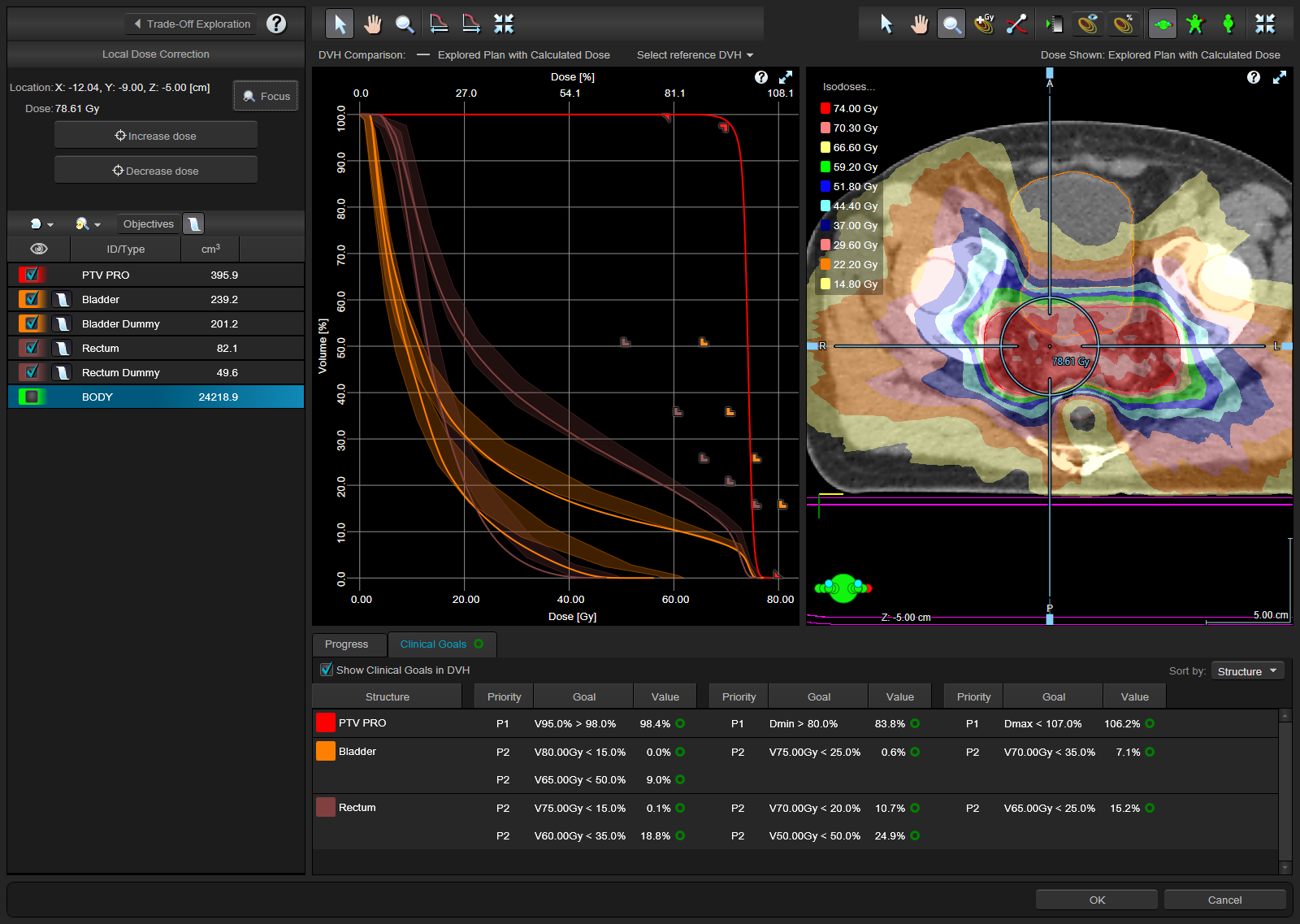
Our example plan has a rectum dose which is a little high (while still in the band of the DVH estimation), so we focus on reducing rectum dose, by moving the Rectum slider to the left, which means lower doses:
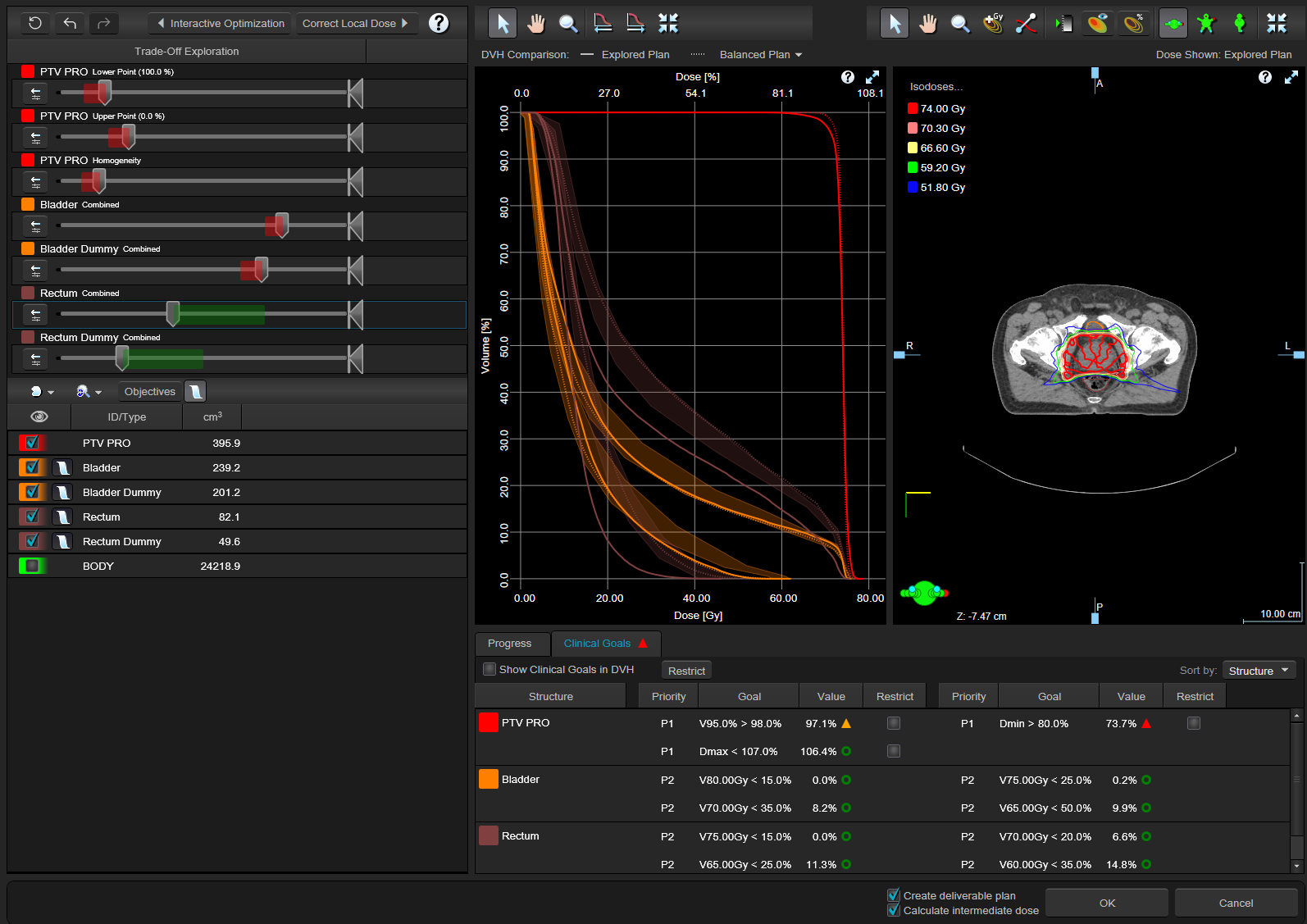
While the Rectum slider is moved with the mouse, all other sliders react and show some kind of contrail, to indicate the direction of movement. The original DVH curves are kept as dotted lines, while the full curves are the actuals. The clinical goals of the PTV tell us that the change was a little too much. We are still on the Pareto surface, so in a sense all plans we create by moving sliders are "optimal", but this does not mean that they automatically fulfill our clinical goals.
A good result can be achieved with a more careful move of the Rectum slider:
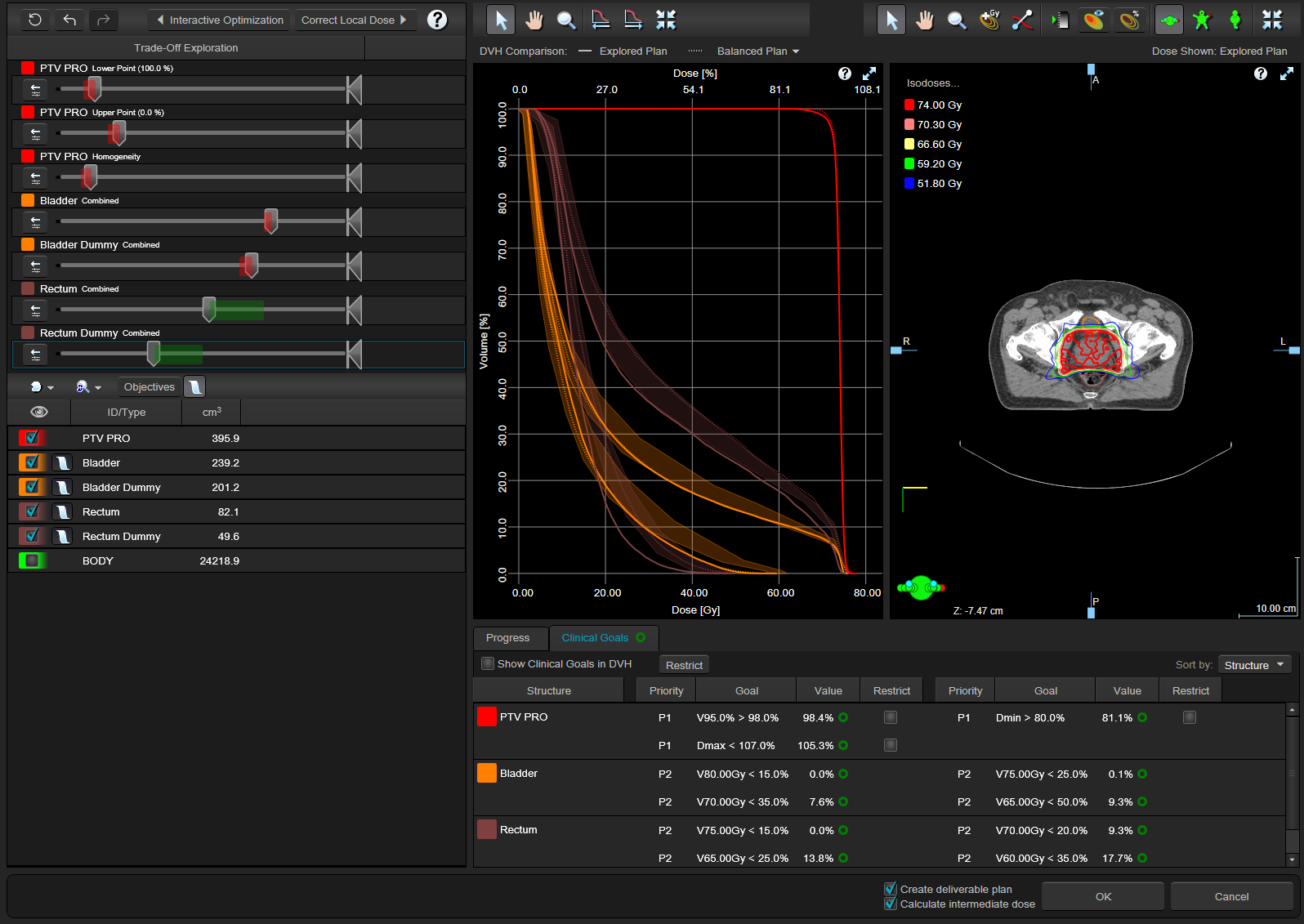
Now all the goals are green, and we have shifted the rectum curve from the upper edge of the DVH estimation band to its lower edge. Remember that we started off with a plan that we already considered as "good".
The possibility to restrict the changes to plans which do not violate the clinical goals of the PTV comes in handy. All we have to do is check all "Restrict" boxes in the Clinical Goal section for the PTV:
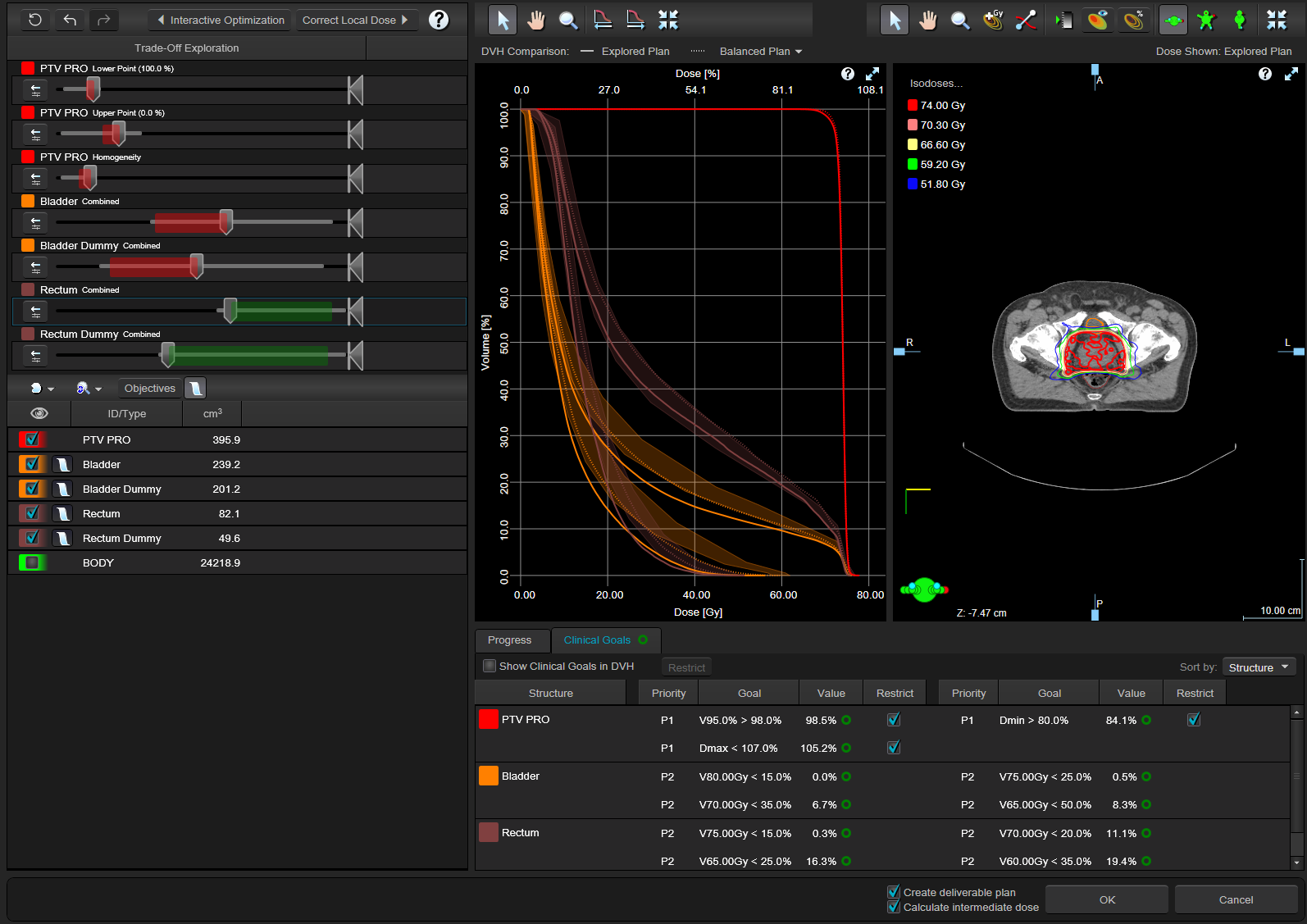
The restriction limits the travel range of all sliders, so that it is no longer possible to violate PTV goals.
It is interesting to observe how the other sliders react if one slider is moved. Organs and their "dummy" versions (which don't overlap with targets) move more or less in sync, because they represent the same organ, with the dummy being cropped. When the rectum is forced down too far, the bladder starts to go up. This reflects the fact that somehow the PTV has to receive a certain dose, so limiting one sector of entrance angles puts more loads on the other angles.
After playing around for a while with the sliders we have settled on a nice spot on the Pareto surface and click OK. This starts the creation of the deliverable plan, MCO1.
As with the manually optimized plan, MCO1 has a small hotspot outside the PTV. Local Dose Correction was used to correct this.
Results and Discussion
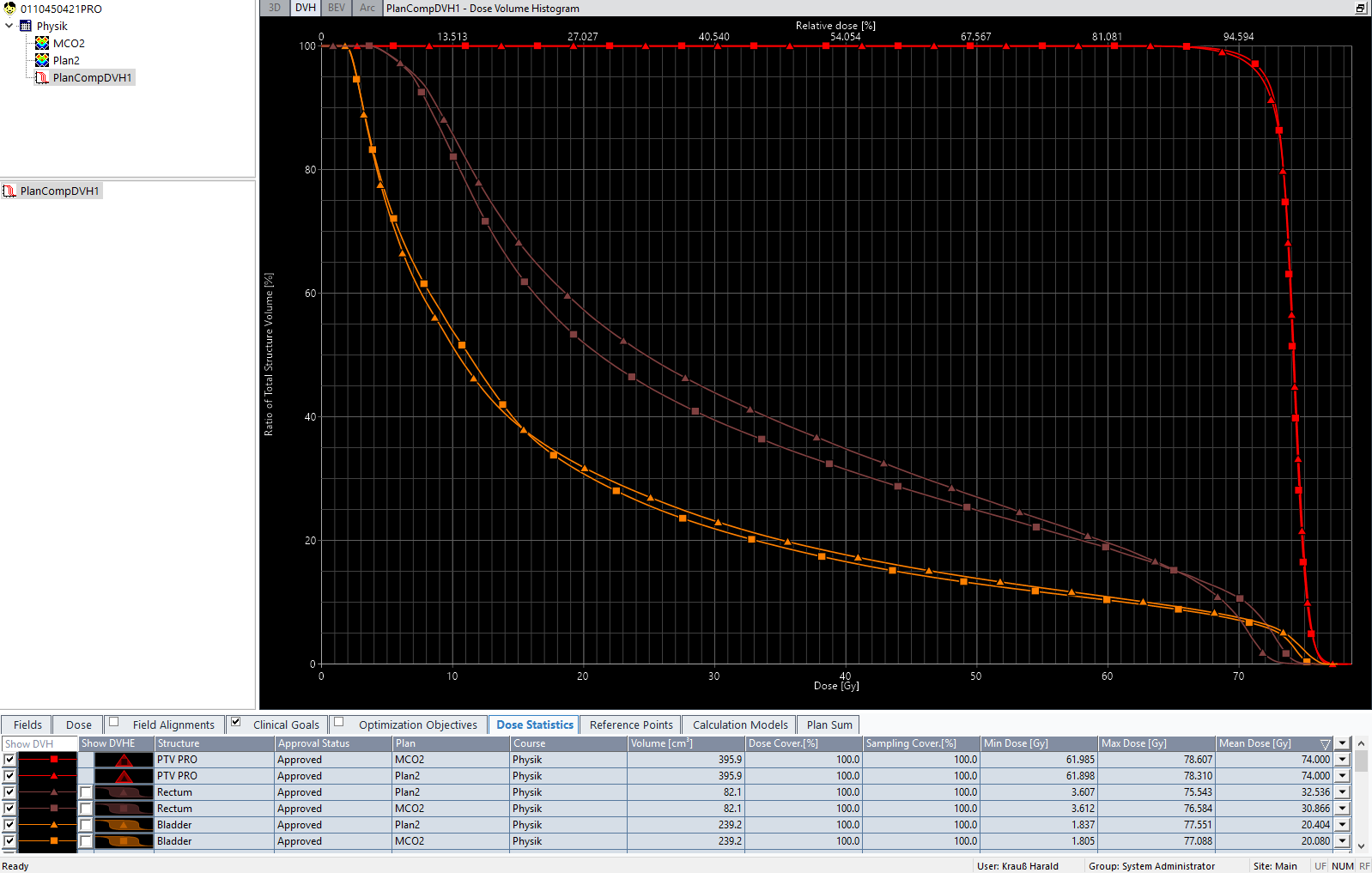
How does plan MCO2 compare to the manually optimized plan, Plan2? In the example, we have focussed on rectum dose. DVH comparison shows that in the MCO plan (squares), rectum mean dose is lower by 1.67 Gy compared to the manually optimized plan (triangles). But also bladder and PTV are slightly better in MCO2:
Is the MCO based plan always better? At least, we can say this: Let's assume we use MCO and discover that there is "potential" for further OAR dose reduction. If we would now go back to manual optimization, apply the proper dose objectives and reoptimize the plan, we would get the same plan quality as with MCO. But the question is this: without MCO and trade-off exploration, would we have discovered the potential in the first place? For the example prostate plan, one could argue that for the balanced plan, the potential could be guessed from the hot position the Rectum DVH curve has inside the DVH estimation band. But this is a rather weak argument. A reoptimization study which involved model plans for our DVH estimation models revealed that in the past we sometimes missed opportunities2.
This probably describes best the benefits of MCO in our work: to discover potentials. By using trade-off exploration, we sometimes reach areas of the solution space which would otherwise remain undiscovered. And if we are lucky, we can keep on going and finalize the plan until it can be delivered to the patient. Many manually optimized plans are not yet on the Pareto surface.
Of course, there is always room for improvement. The clinical goal numbers for instance which are displayed when we exit Trade-Off Exploration are not exactly the same, to one digit after the comma, as the numbers which we get in the final, 3D dose calculated plan. They can be off by 0.5%, sometimes even more. There are sure different sampling algorithms involved, so the best way to avoid clinical goals which are green in Trade-Off Exploration but red in External Beam Planning is probably to leave some room for the numbers.
Notes
1 The Pareto surface is a concept in multi-objective optimization. Any treatment plan balances the different trade-off objectives regarding tumor coverage and sparing of OARs in a certain way. The treatment plan balances these objectives in an efficient manner if no trade-off objective can be improved without worsening some other trade-off objective. The entirety of treatment plans that are efficient with respect to certain, fixed trade-off objectives is called the Pareto surface. (Eclipse Photon and Electron Algorithms Reference Guide, August 2019).
2 Keep in mind though that we are talking of small improvements in plans which are already very good.